The yard-work syndrome
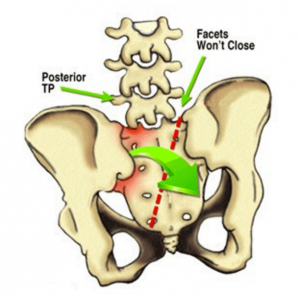
Now that summer is upon us, I’m beginning to see more clients complaining of bending and twisting back pain. In most people, the lumbar spine and sacrum are pretty stable during forward bending and lifting, but not so when sidebending and/or rotation are added to the equation. Sacroiliac joint biomechanics is complex and controversial, so I will limit our discussion to one very painful condition (treated in the video below) termed a left-on-right backward sacral torsion (Fig. 1).
To simplify sacral torsion biomechanics, please try these two palpation exercises:
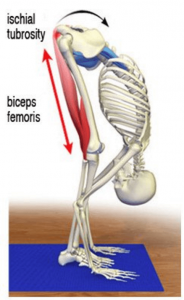
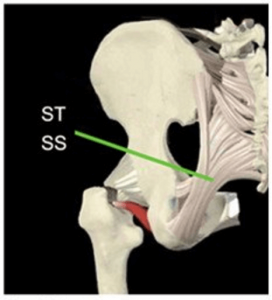
1. Stand and place the fingers of each hand along the superior border of your sacrum. Forward bend the trunk and feel this bone push back at you. The sacral bases are actually moving posterior and a little bit superior, but you won’t feel the headward movement much, because the sacrotuberous and sacrospinous ligaments (and slips of biceps femoris) are tugging on the sacrum from below (Fig. 2a & Fig. 2b). This musculoligamentous bracing action allows all the lumbar facets starting at L5, to glide forward on their inferior neighbors so we can perform activities such as leaning over to tie a shoe.
2. Stand in a comfortable posture maintaining a natural lumbar lordosis. Place your fingers or thumbs on the lower lumbar transverse processes (TPs) and sidebend left. You should feel these bony knots push back into the fingers of your right hand. Now, forward bend your trunk to end range and again sidebend left. In an optimally functioning spine, the TPs should rotate back into the fingers of your left hand. When sidebending and rotation couple to the same side during forward bending, osteopaths label this “non-neutral” mechanics.
Typically, L5 and the sacrum couple to opposite sides, i.e., left lumbar sidebending causes right sacral sidebending, etc. But, when the lumbar spine is flexed, sidebent and rotated left, the sacrum also sidebends and rotates left. The potential damage is amplified when the person attempts to lift an object with the spine and sacrum both ‘cocked’ the same direction. This motion is a biomechanical challenge for the intervertebral discs, spinal ligaments, facet joints, and deep core musculature, and a major reason the L5-S1 disc is the most operated in the body.
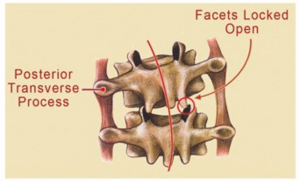
To make matters worse, when the person begins straightening up, the L5 facet cartilage on the right sometimes jams against the top edge of the sacral facet cartilage; a condition called facet nipping (Fig. 3). The downward force of the left rotating L5 buries the right sacral base and locks the lateral border of sacrum into left sidebending and left rotation (along a right oblique axis) (see Fig. 1). With the left sacral base and inferior lateral angle jacked up posteriorly, and driven inferiorly into extension, stabbing pain is often immediately felt in the low back, SI joint, and/or down the leg, like sciatica.
Prone testing reveals a short left leg, posterior L5 transverse process on the left, and absolutely no spring in the lumbar spine or left SI joint. But backward sacral torsion assessments are usually pretty easy to make via history, and by watching the client try to walk and stand erect. In chronic cases, an orthopedic workup helps eliminate the possibility of disc and/or ligament damage. However, most cases respond well to various forms of manual and movement-based therapies.
I’ve experimented with many soft-tissue SI joint techniques over the years, but the ones Paul Kelly and I teach in the new “Motion Is Lotion” videos seem to be the simplest and most effective for relieving this sometimes-debilitating condition. To reduce damage and prevent reoccurrences, length-strength muscle imbalances and aberrant motor control patterns must be addressed through tailor-made corrective exercises.
One note of caution: Because the client can’t completely extend through the posterior chain, many therapists recommend hyperextension maneuvers like the cobra or McKenzie-type exercises, prior to the torsion correction. This type of retraining only serves to worsen the problem, as excessive compressive and torsional forces wreck havoc on facet and SI joints. For an in-depth study of sacroiliac dysfunctions, please read Jerry Hesch’s “Sacral Torsion About An Oblique Axis” chapter in my Dynamic Body book. Much Thanks!
On sale this week only!
Save 25% off the Upper Body Course!

NEW! Enhanced video USB format!!!
Learn unique approaches to work with the shoulder girdle, arms, neck, and torso, this course will prepare you to relieve painful myoskeletal issues in the upper body. Through video demos and animation, you’ll learn to identify several compensatory movement patterns and their associated reflexogenic pain. With this understanding of where the true source of problems arise, you’ll be able to develop highly effective treatment protocols and deliver lasting results. This course provides you with the skills you need to confidently relieve pain issues in the upper body. (20 CE)
Bonus: When you order the Home Study version, get the eLearning course and and an additional 2CE Ethics eCourse for free!
Save 25% off the Upper Body Course this week only. Offer expires Sunday, March 1st. Click the button below for more information and to purchase the course for CE hours and a certificate of completion to display in your office.







