Clinical Implications for Manual Therapy
Understanding whether you’re dealing with true adhesive capsulitis versus a more general frozen shoulder condition helps guide your treatment approach and timeline expectations.
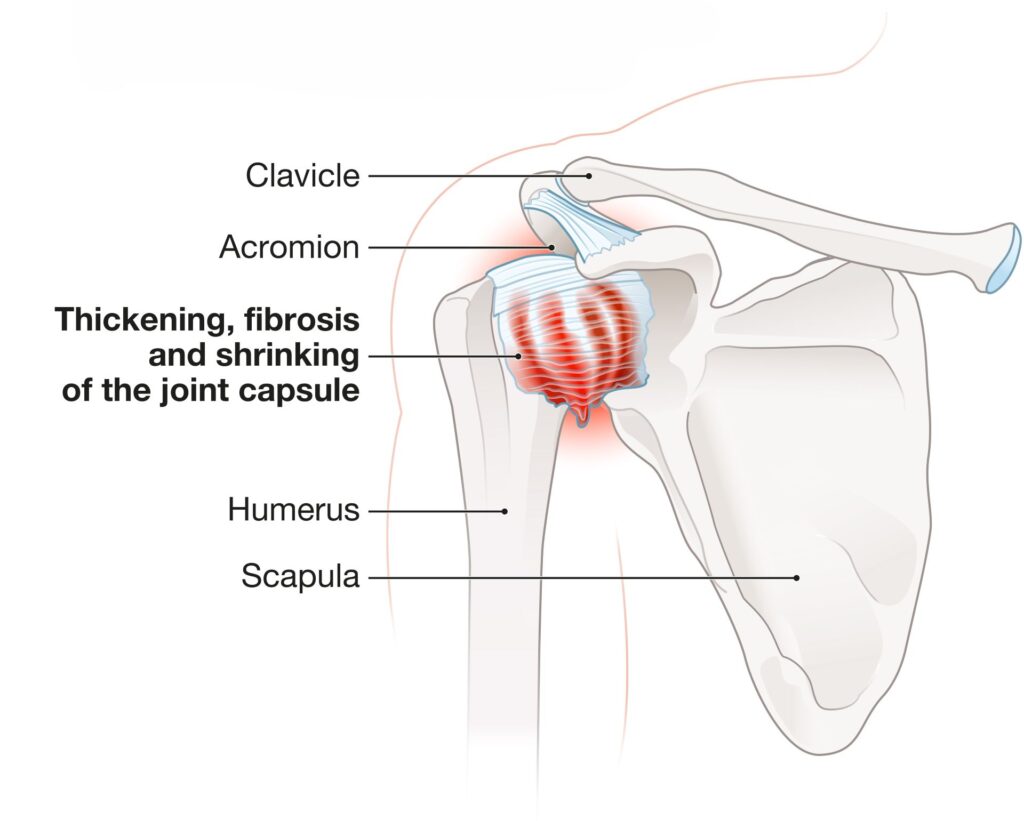
True adhesive capsulitis typically progresses through three distinct phases: the painful freezing phase (2-9 months), the stiff frozen phase (4-12 months), and the gradual thawing phase (5-24 months). Clients with this condition often benefit from gentle joint mobilization techniques, capsular stretching, and patient education about the natural progression of their condition.
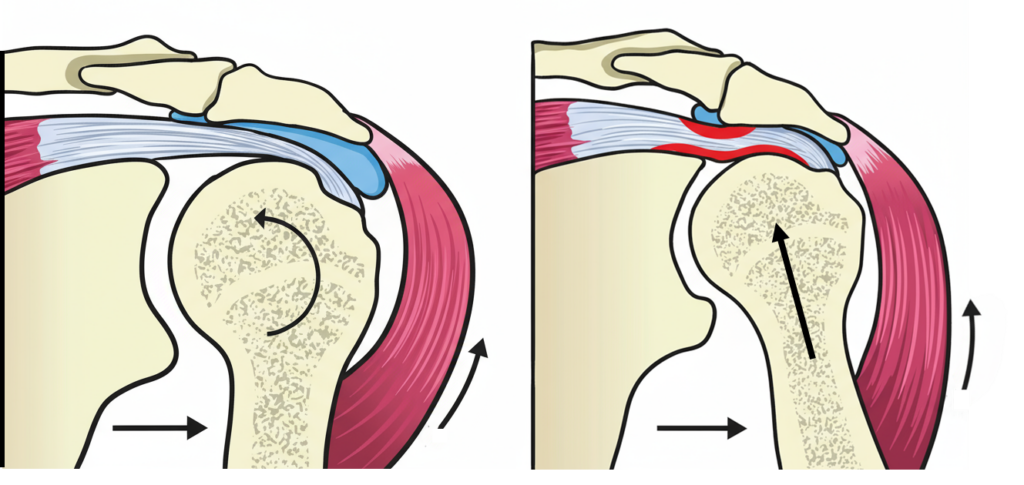
General frozen shoulder conditions caused by muscle guarding, impingement, or minor adhesions may respond more quickly to targeted soft tissue work, corrective exercises, and addressing underlying postural imbalances that contribute to the restriction.
In both cases, myoskeletal alignment techniques that focus on improving joint mechanics and restoring optimal movement patterns can be highly effective. The key is matching your intervention to the underlying pathology and setting realistic expectations for recovery.
Remember, successful treatment of shoulder restrictions requires a balance between addressing local joint mechanics and considering the broader kinetic chain adaptations that develop over time. By understanding the difference between frozen shoulder and adhesive capsulitis, you can provide more targeted, effective care for your clients while avoiding the frustration that comes from treating symptoms without addressing root causes.
For more information on myoskeletal alignment techniques for shoulder conditions, explore our comprehensive course offerings and additional blog posts on treating upper extremity dysfunction.
References
- http://my.clevelandclinic.org/orthopaedics-rheumatology/diseases-conditions/frozen-shoulder-vs-adhesive-capsulitis.aspx
- Andrew S. Neviaser, MD, and Robert J. Neviaser, MD. Adhesive Capsulitis of the Shoulder, Journal of the American Academy of Orthopedic Surgeons, September 2011. Vol. 19. No. 9. Pp. 536-543.