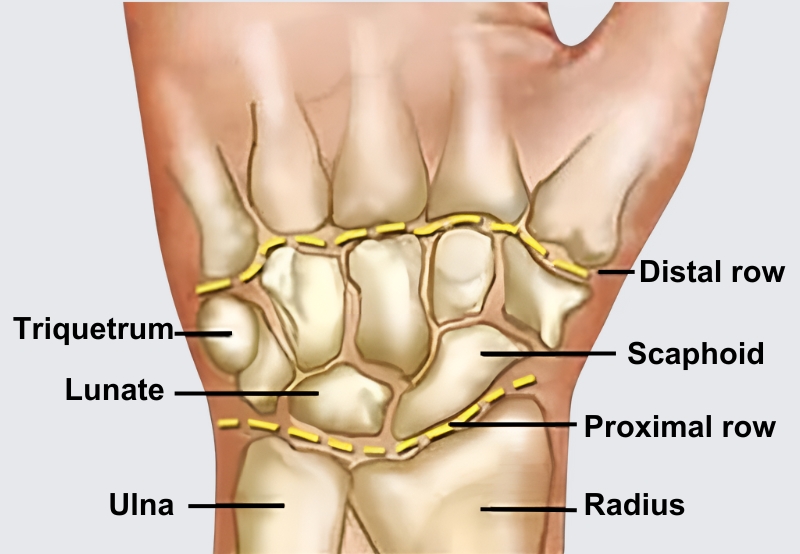
Artists, bodyworkers, computer programmers, and writers are among those who suffer from overuse syndromes such as carpal tunnel syndrome (CTS). Although most of us have developed hands-on skills for relieving median nerve compression as it passes under the transverse carpal ligament, I believe the treatment can be enhanced. By adding simple nerve and joint gliding techniques, inflammation, which arises as tendon and nerve sheaths glide across rigid carpal bones, is often reduced (Image 1.).
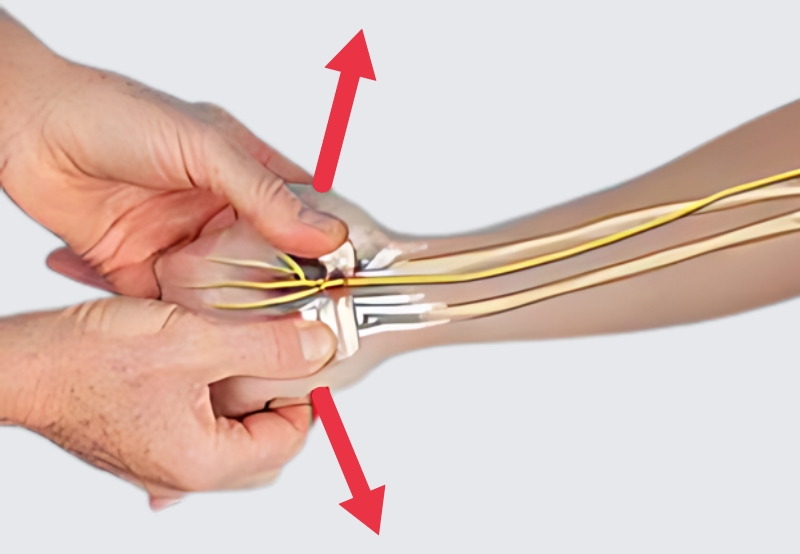
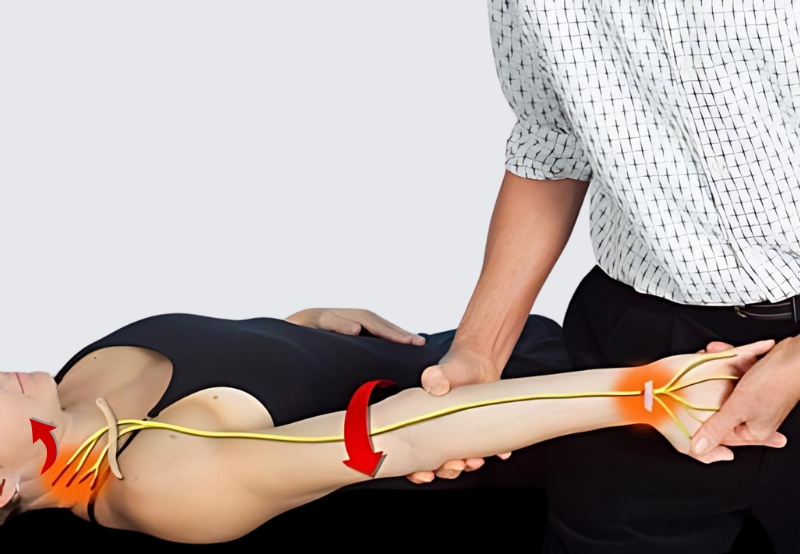
A 2015 study published in The Journal of Pain reported physical manual therapies that included central nervous system desensitization maneuvers were effective in improving CTS pain.1 By restoring proper carpal joint positioning, massage helps lower intra-tunnel pressure and boosts median nerve glide. I’ve found gentle carpal stretching facilitates longitudinal nerve excursion and reduces protective guarding in the arm flexor muscles. To test this hypothesis, let’s first assess and correct the most common carpal bone fixation (lunate), then get the median nerve gliding, and retest.