Ideal shoulder girdle balance requires that some muscles act as stabilizers and others as mobilizers, depending on joint position and movement required for the particular task. A perfect balance of mobilizers and stabilizers results in optimal alignment, or joint centration. Think of joint centration like the wheel on a car. If the center of rotation is aligned with the center of the hub, it will deliver the most efficient performance. Conversely, when this neutral position becomes misaligned, the wheel spins incorrectly and can result in future mechanical problems. We commonly see this in upper crossed syndrome (UCS) postures where slumped shoulders and a head-forward carriage lead to scapular winging and decentration of the glenohumeral joint (Image 1).
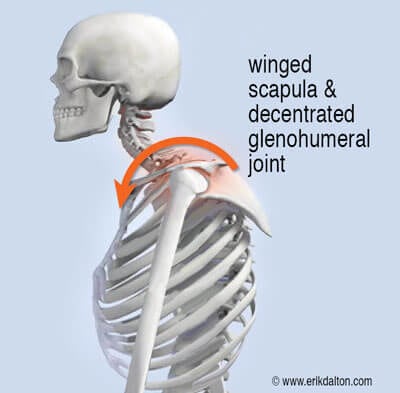
Although researchers have not been able to correlate rotator cuff impingement with suboptimal postures such as upper crossed syndrome, my experience is that it plays a major role in many rotator cuff tendinopathies—particularly in those who perform overhead activities. Try this experiment: Stand in a military posture with shoulders back and chin tucked. Close your eyes and abduct your arms out to the side and over your head as far as comfortable. Notice the range of motion during this maneuver. Next slump into a forward head posture, chin jutting out and arms internally rotated. Close your eyes and raise your arms overhead as far as comfortably possible. You should have 50% less range of motion through the shoulder girdle and most will feel strain in the rotator cuff at about 90 degrees. I’m not talking about pain here; I’m talking about loss of function.
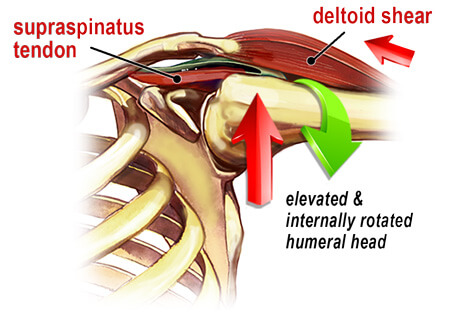
Deltoid Shear
A key task of the cuff muscles is to maintain the head of the humerus centrated within the glenoid fossa (concavity compression), while imposing an inferiorly directed force to the humeral head. In those with rounded shoulder postures, the glenoid fossa’s mechanical axis of rotation is altered, causing the brain to activate muscles that are typically at rest, such as upper traps, levator scapula, pec minor and the deltoids. Postural overdevelopment of these muscles undermines rotator cuff stability, causing a ‘deltoid shear’ that can elevate and compress the humeral head into the top part of the glenoid fossa (Image 2.). In this position, arm abduction to 90° is more likely to squash the supraspinatus tendon against the acromion, causing micro-fraying, fibrosis, and possible tendinosis.
Poor posture may start as a “tissue issue” due to tension, trauma, or overuse injuries. Eventually, however, it manifests as a sign of functional weakness in the brain’s hardware. This weakness may stem from faulty peripheral input, inaccurate cortical processing, flawed output, or a combination of these factors. Any alteration of joint function influences muscular function thus producing a self-sustaining chain reaction. To understand the fine control of motion, the separate activity of individual muscles is not as important as their coordinated activity within the different movement patterns.
Passively stretching tight, inert capsular tissue may resolve only part of the stiff shoulder problem. Active motion applied frequently to the restrictive tissues reinforces available ROM gained during joint mobilization. Let me stress again that mobilization with movement is a highly recommended treatment technique. Active movement psychologically reinforces to the client that she can move the arm through a greater range of motion. Physiologically, active movement not only assists in healing collagen tissue allowing it to align itself along normal stress lines, but also aids in restoration of normal strength. Active movement also nourishes articular cartilage and enhances repair of damaged tissues. In Images 3 and 4… I demonstrate myoskeletal techniques for addressing upper-crossed syndromes, deltoid shears, and rotator cuff injuries. Once proper glenohumeral mobility is restored, home retraining advice should include exercises for core stability, scapular stabilization, and rotator cuff strengthening.


Remember: mobility first
Refrain from advising muscle-strengthening exercises for joints that are not moving freely. This can lead to cartilage degradation and ultimately capsulitis or osteoarthritis. When massage and movement therapists successfully restore length-strength myoskeletal balance, tissue lubrication improves and the transmission of nerve impulses becomes more efficient. Better proprioceptive neural feedback enhances motor control and reduces injury in clients suffering chronic rotator cuff pain.
The reflexogenic relationship of muscles and joints is at the core of the myoskeletal method. Biomechanical analysis of specific joints is not difficult and can help rule out suspected soft tissue injuries. In skilled hands, joint mobilization is a crucial and effective element in injury prevention.