Synergistic may be defined as “acting together to enhance the effect of another force.” Therefore, if muscles perform the same task at a particular joint, they are termed synergistic. Synergistic dominance occurs as “helper” muscles are recruited to take over function when a “prime mover” muscle fails, much like when a football coach calls in the substitute players when a key player is injured. These synergistic stabilizing muscles are designed to help, but not be primary contributors, to a particular movement.
Reciprocal inhibition is often the precursor to synergistic dominance. For example, in forward-head postures, the client’s suboccipitals are often maintained in a hypercontracted state as they battle gravity to keep the eyes level with the horizon. As the head cocks back and moves forward on the neck, the antagonist longus capitis muscles – which bind the anterior surface of the upper cervical vertebrae to the occipital base, become overstretched and weak (Fig. 1). Sensing the longus capitis muscles can no longer carry out their duty as primary head-on-neck flexors, the brain calls on the powerful sternocleidomastoids (SCMs) as pinch-hitters (Fig. 2).
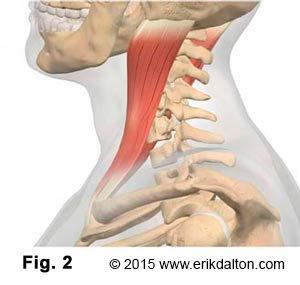
The SCMs are reliable neck flexors when allowed to fire in proper order. However, they serve as poor subs for longus capitis due to their insertion at the mastoid process. When reciprocally weakened, longus capitis muscles give way to powerful SCMs which are forced to fire first, causing the head to cock back into extension (not flexion). Neural and vascular structures embedded at the posterior O-A joint aren’t so happy with the excessive compression. Therapists may choose from several strategies to unwind this common head-on-neck imbalance pattern.
When the neck’s normal firing-order sequence is disrupted, synergistic muscles can torsion and compress facet joints, causing chronic degenerative conditions such osteoarthritis, migraines and dowager’s humps. The brain compensates by layering the area with protective spasm, which perpetuates pain-spasm-pain cycles as the neck’s firing order pattern is further disrupted. Fortunately, the trained eye can usually spot synergistic dominance patterns. The client’s gait may reveal certain body parts that appear frozen in time, as chronically embedded compensations have caused the brain to sacrifice complexity of movement for stability. Fortunately, simple tests help determine if synergistic dominance exists at a particular joint.
Neck Flexion Test
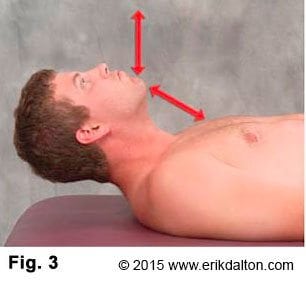
Forward bending of the head and neck with the client in a supine position should initiate the following firing-order sequence: longus capitis, longus colli, SCMs and anterior scalenes. The deepest intrinsic muscles must fire first starting with longus capitis (flexing the head on the neck) followed closely by longus colli which initiates the beginning of neck flexion. Anterior scalenes and SCMs can then join forces to produce smooth head-and-neck flexion. The most commonly seen substitution pattern (SCMs, anterior scalenes, longus colli, and longus capitis) causes the chin to reach toward the ceiling rather than tucking into the chest during the first two inches of flexion efforts (Fig. 3). The neck flexion test alerts the therapist as to which musculofascial tissues need lengthening and which must be strengthened.
Tension-length imbalances are usually easy to fix. The video below demonstrates one of my favorite techniques for releasing adhesions and contractures in the sternocleidomastoid muscles and their accompanying fascia. By performing the head-raise test before and after each neck session, aberrant substitution patterns can be easily identified and corrected.
Today’s manual therapist must recognize that musculoskeletal pain syndromes in the cervical spine cannot be viewed independently from the functional status of other body structures. Therapists must assess and treat the neuromyoskeletal system as a whole, and give consideration to muscle dysfunction as it relates to the functional status of the whole motor system, including articular and nerve structures.
On sale this week only!
Save 25% off the Upper Body Course!

NEW! Enhanced video USB format!!!
Learn unique approaches to work with the shoulder girdle, arms, neck, and torso, this course will prepare you to relieve painful myoskeletal issues in the upper body. Through video demos and animation, you’ll learn to identify several compensatory movement patterns and their associated reflexogenic pain. With this understanding of where the true source of problems arise, you’ll be able to develop highly effective treatment protocols and deliver lasting results. This course provides you with the skills you need to confidently relieve pain issues in the upper body. (20 CE)
Bonus: When you order the Home Study version, get the eLearning course and and an additional 2CE Ethics eCourse for free!
Save 25% off the Upper Body Course this week only. Offer expires Sunday, March 1st. Click the button below for more information and to purchase the course for CE hours and a certificate of completion to display in your office.







