Introduction
Pelvic pain can be frustrating because it often feels local, but the pattern is rarely isolated. A client may point to one sacroiliac joint, one hip, one side of the low back, or the pubic symphysis and say, “It hurts right here.” But the pelvis functions as a ring. When one part of the ring stops moving well, the rest of the ring has to adapt.
That is why direct pressure on the painful spot is not always the best choice. In many cases, the painful joint is already being protected by the nervous system, and the surrounding muscles are already hypertonic. Instead of compressing painful tissue, these techniques use gentle leverage, rhythmic motion, and a contract-relax effort to provide novel stimulation. The goal is to reduce guarding, improve joint motion, and help the pelvis return to balanced load transfer.
Anatomy and Biomechanics
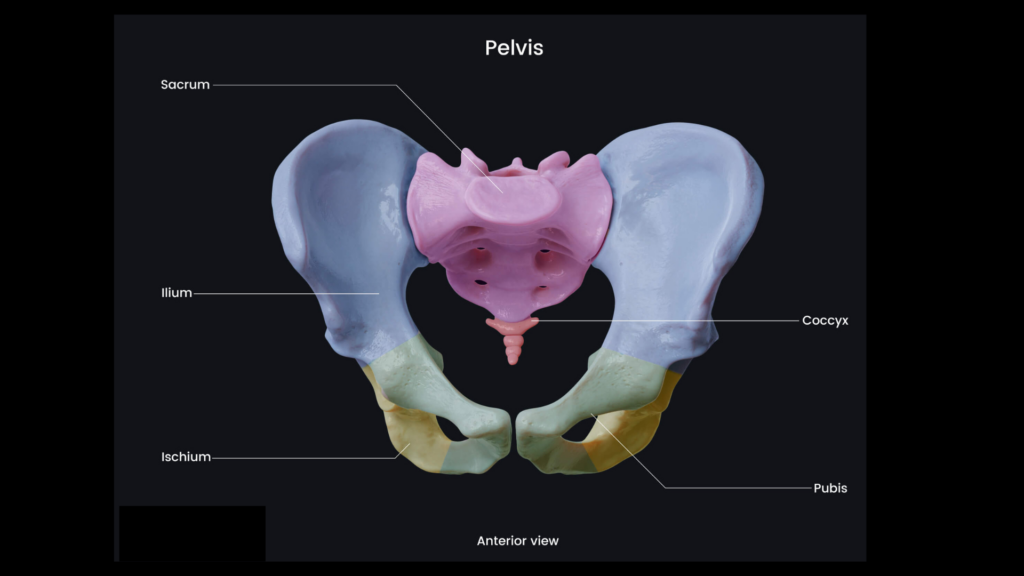
The pelvis is a ring-shaped structure formed by the two innominate bones, the sacrum, and the coccyx. Each innominate bone is made of the ilium, ischium, and pubis. Posteriorly, the sacrum joins the ilia at the sacroiliac joints. Anteriorly, the pubic bones meet at the pubic symphysis. Together, these joints create a strong but adaptable ring that transfers load between the spine and lower limbs.
The pelvis has two primary biomechanical roles: stability and force transmission. Body weight moves from the lumbar spine into the sacrum, across the sacroiliac joints, through the acetabula, and into the femurs. Ground reaction forces travel upward through the femurs and hips into the pelvic ring. Efficient movement depends on balanced load sharing between the right and left sides.
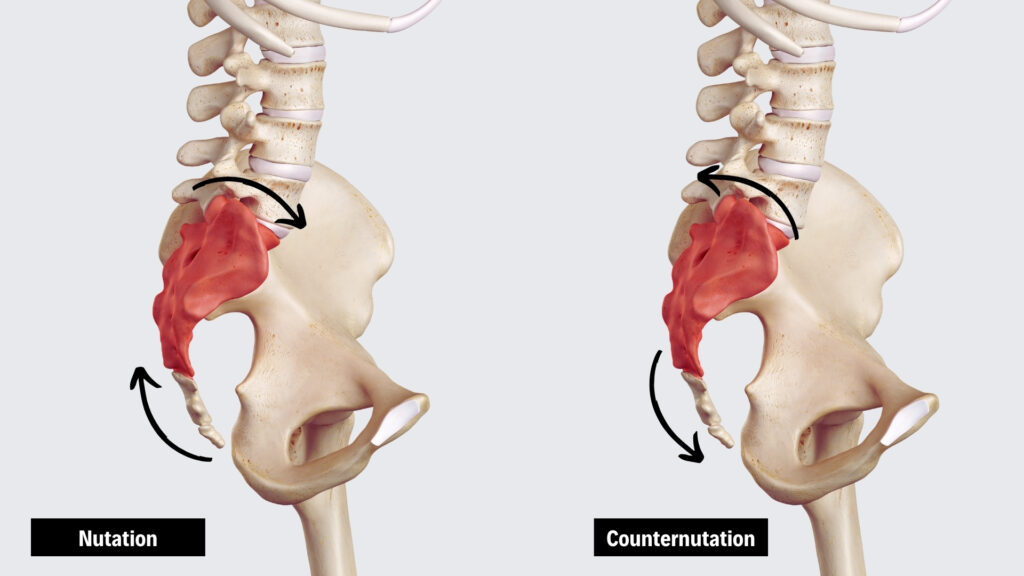
In an unguarded pelvis, the SI joints and pubic symphysis work together as part of a mobile ring. The sacrum nods between nutation and counternutation, while the pubic symphysis gives with tiny amounts of compression, separation, shear, and rotation. When one innominate rotates forward and the other back, as in gait, the symphysis absorbs that difference as a slight vertical shear between the two pubic bones.
Nutation and Counternutation
Nutation occurs at the SI joints when the sacral base moves anteriorly and inferiorly between the ilia. This motion tensions the sacrotuberous and sacrospinous ligaments and helps stabilize the SI joints during load-bearing activities such as standing, walking, rising from a chair, and lifting. In these moments, the pelvis needs enough stiffness to transfer force efficiently between the legs and spine.
Counternutation reduces the tension of the sacrotuberous and sacrospinous ligaments, allowing the sacral base to move posteriorly and superiorly as the pelvis accommodates flexion, sitting, and changes in load.
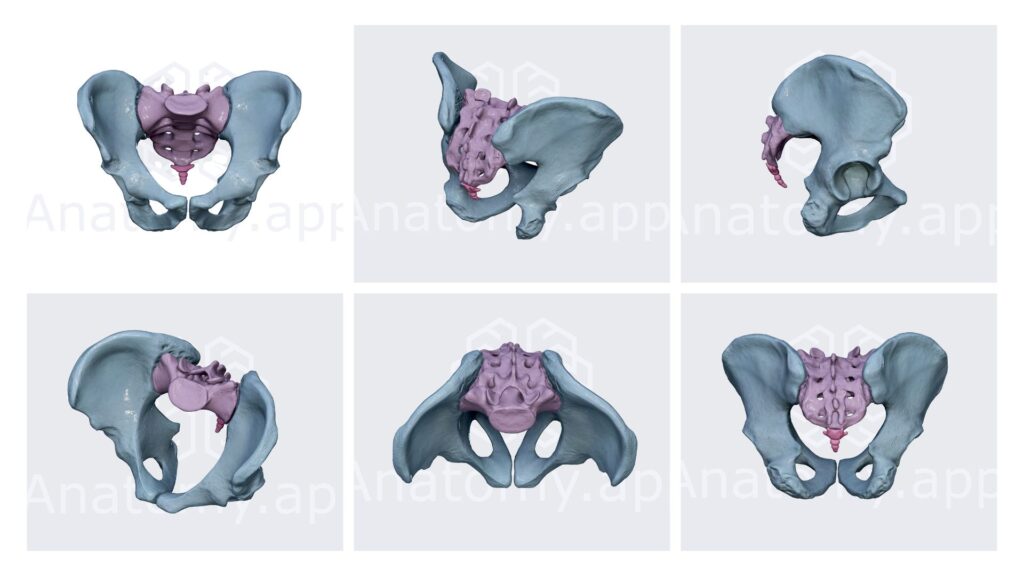
Take a moment to watch the animation of the pelvis used with permission from anatomy.app. As nutation, counternutation, and the give of the pubic symphysis cycle together rhythmically, the pelvis seems to breathe.
Guarding Against a Perceived Threat
Now introduce any source of irritation, pain, or perceived threat. Maybe a structural asymmetry like a leg-length discrepancy is overloading the hip joint and irritating the capsule. Maybe a past injury has taught the brain to expect that a movement will hurt. Maybe the joint’s position is signaling instability and danger. In any of these situations, the nervous system is likely to guard the pelvis by restricting motion.
This guarding is meant to create safety, but it can also interfere with the timing and contribution of the muscles that normally stabilize joints. Some muscles under-contribute, while compensating muscles overwork.
Over time, this compensation can pull the pelvis away from neutral. One side may hike, rotate, or shift differently from the other, changing how force is transmitted through the sacroiliac joints, hips, lumbar spine, and lower limbs. The brain then has to manage a pelvis that feels less symmetrical and less predictable. That asymmetrical position becomes one more reason to guard, and the original protective strategy begins to reinforce itself.
Our training in massage therapy might encourage deep soft-tissue work on the area of pain. But applying forceful pressure to a guarded region can increase protective tone rather than reduce it.
A more effective strategy is to provide input that is controlled, pain-free, and nonthreatening. Gentle, rhythmic movement can alter sensory input to the nervous system without provoking further protection. As threat perception fades, the nervous system can reduce protective tone and improve the firing patterns and contribution levels of the pelvic muscles. This is the central principle behind these techniques.
Integrate these techniques into your bodywork sessions and check out Case Study 7 (Pelvic Biomechanics) in the Motion is Lotion course. These methods deliver mechanical and sensory input to the pelvic ring to reduce guarding in the guarded pelvis.
Precautions & Contraindications
Acute Injury: Acute trauma, sprains, strains, or recent surgery.
Pregnancy & postpartum: The pelvic ring is already loose and often tender; it doesn’t need more mobility. Leave these techniques out of the massage.
Hip or knee replacement: This sequence loads the hip and knee through the leg. Modify significantly or leave these techniques out of the massage.
Osteoporosis or fragile bone: Leave these techniques out of the massage.
Hypermobility or unstable joints: There is already too much motion; mobilizing can make it worse.
Inflammatory joint conditions: For example, ankylosing spondylitis, RA in flare — don’t mobilize an inflamed joint.

Arm-Lock SI Joint Mobilization
We’ll use the Arm-Lock Maneuver to take the flexed hip through rotation, abduction, adduction, compression, and distraction. We’re treating every plane of movement with low-threat impact, signaling to the brain it’s safe to reduce guarding.
The client is supine with their right knee flexed and their right foot resting flat on the table. Stand on the client’s right side and use an arm-lock position by snaking your right arm over and through the popliteal space. Brace the client’s anterior thigh with your left hand so the flexed hip can be gently internally and externally rotated, abducted and adducted, and alternately distracted and compressed. First, pull the client’s thigh to distract the hip and encourage posterior rotation of the right ilium. Then push the thigh toward the pelvis to compact the hip and encourage anterior rotation of the right ilium. Repeat this distraction and compaction two or three times. With the hip distracted, ask the client to pull their hip toward the table against your resistance for a count of 5, then relax. After the client relaxes, lean your body weight back to distract the hip and decompress the restricted hip capsule. Repeat as needed, keeping the movement pain-free and controlled. To avoid contact with breast tissue, place the client’s knee in your armpit instead of using the full arm-lock position.

Superior Pubic Shear Technique
Take a moment to visualize the video showing the coordinated movements between the SI joints and pubic symphysis during nutation and counternutation. If the pubic symphysis is stuck with one pubic bone slightly higher than the other, the pelvic ring can’t move the way it should. This technique sets up a closed-chain contract-relax using the adductors and abductors as levers on the two pubic bones.
The client is supine with both knees flexed and both feet flat on the table, about shoulder-width apart. Move the client’s knees slightly apart, then place your right arm between them to provide resistance. Ask the client to press through their heels and lift their hips into a bridge while squeezing their knees together against your resistance. Have the client slowly lower their pelvis back onto the table while maintaining gentle adduction pressure into your arm. Next, bring the client’s feet and knees together, and place your arms along the outer sides of both knees. Ask the client to abduct their knees against your resistance as they bridge up and slowly lower back down. Repeat the adduction bridge and abduction bridge three to five times, keeping the effort controlled and pain-free.

SI Joint Jostling
This technique involves a rhythmic pull-and-resistance mobilization of the SI joint that feels safe and enjoyable to the nervous system.
The client is prone with the left leg slightly off the table. Place the client’s left foot between your knees so you can control the leg with your lower body. Practice pulling the client’s hip inferiorly by dropping your body weight back. Place your right hand on the inferior border of the sacrum and brace your left hand on top of your right. Create a counterforce by using your legs to traction the client’s left leg while your hands resist at the sacrum. Once the counterforce is established, rhythmically pull and push through the leg to gently jostle and mobilize the sacroiliac joint. Keep the motion steady, pain-free, and within the client’s tolerance. If placing the client’s leg between your knees is uncomfortable, keep the leg on the table, place one hand on the knee and the other on the sacrum, and gently jostle the joint from that position.

Deep External Rotators Release
Pelvic guarding can cause the deep external rotators to become overworked and hypertonic. This release addresses the soft tissue to relax these muscles.
Turn your client into the prone position. Bring the client’s left knee into flexion and hook your left arm around the client’s ankle. Place your soft right forearm just lateral to the sacrum so you can palpate the deep hip external rotators, including the piriformis. Gently move the client’s femur into internal rotation by pushing the lower leg away from you, which brings the external rotators to their first restrictive barrier. As you palpate the tissue, assess for increased tone or restriction. Ask the client to gently push their ankle against your resistance for a count of 5, then relax. After the client relaxes, bring the hip into the new internal rotation barrier while continuing to work the piriformis and the surrounding external rotators with your forearm. To enhance the release, lift the client’s hip slightly with your left arm while your right forearm drags the external rotator tissue inferiorly. Repeat as needed, staying within a pain-free range.
In Closing
The techniques taught here aim to improve the biomechanics between the joints, muscles, fascia, and nervous system to encourage easier hip motion and better pelvic symmetry. When movement feels safer and more predictable, the nervous system can reduce guarding, and muscles can contribute at the right levels to unguard the pelvis.