by Gil Hedley, Ph.D.
Read this very informative chapter in its entirety in the Dynamic Body Textbook
The book is also a part of the 32 CE Lower Body Home-Study
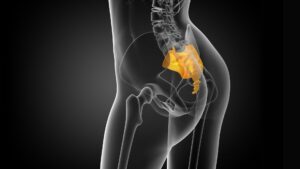
Notes on Distinguishing Normal and Abnormal Fascial Adhesions
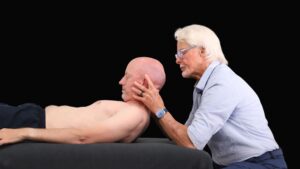
In the early years of my dissection studies, I was an active practitioner of structural integration. I believed that if I used my hands to “differentiate” my clients’ tissues, I could help them to experience freedom of movement more fully. Therefore, it is not surprising that I approached cadavers similarly. I would attempt to use my hands to differentiate the different layers of tissue beneath the skin, sometimes with success and sometimes not. Some tissues yielded to fingertip pressure, and I could create space between layers manually, whereas others required a scalpel to separate them.
I was continually surprised by the myriad connections and tissues in the body that were poorly described, or – more often – not accounted for at all by the anatomy flash cards and books. Tom Myers had made it clear to my classmates and me during our Rolfing® pre-training, back in 1991, that “the map is not the territory,” and he was correct beyond my imaginings. Dissection was teaching me that the map was missing continents! Continuities that spanned regions, vast amounts and different types of fascia, as well as the transitional relationships between one tissue texture and another were in fact “all present,” but simply not “accounted for.”
Now, facing such a problem, one strategy would be simply to cut away all the tissue that isn’t in the book, and focus on what’s “supposed to be there.” That is pretty much the strategy of dissection for medical students, who are not going to waste a lot of their severely over-taxed time fumbling with matters outside the curriculum. Make everything look clean and tidy, carve the book drawings out of the tissue, replicate the regional model of separate parts in the unsuspecting cadaver, and consider the resulting prosection a verification of the curriculum.
Lucky for me, I had no teacher in the lab but the cadaver, and I had no test, schedule, or curriculum to which I was beholden. The way I saw it, as a bodyworker and as a somanaut, I was touching the whole person, so I wanted to account for everything that was there materially.
So far in this chapter, I’ve described – with broad strokes – the common, typical, normal tissue relationships, and the variety of qualities inherent in those relations (no attempt to exhaust the subject here).
Now, let’s turn our attention to atypical, anomalous, or pathological relationships. My chapter in Dynamic Body goes on to cover:
* The Search for Normal
* Skin to Superficial Fascia
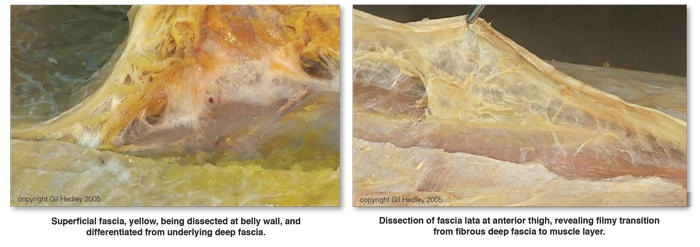
* Superficial Fascia to Deep Fascia
* Deep Fascia to Muscle and Bone
* Within the Muscle Layer
* Filmy Fascia and Muscle Tissues
* Fibrous Fascia and Muscle Tissues
* An Aside on Technique
* Muscle to Bone
* Muscle to Visceral Membranes
* Membranes to Membranes
Veering from “Normal”
* Form Defined by Movement and Stillness
* Scarring
* Holding Patterns
* Visceral Adhesions
Learn more about our Lower Body Home-Study course.