Coccydynia is a term used to describe a malformed or dislocated coccyx and the accompanying growth of bony spurs at this joint. Unlike fractures, which can remodel, sacrococcygeal joint pain can last indefinitely if the inflamed joint is repeatedly forced from its normal position. In cases where inflammatory waste products trigger chemoreceptors and altered sacrococcygeal joint alignment stimulates mechanoreceptors, the brain often locks the area up with reactive muscle spasm to prevent further insult. This is where myoskeletal therapy may help. I encourage you to spark your biomechanical mindset and gain the knowledge necessary to evaluate and treat coccyx pain more thoroughly and confidently.
Pain while sitting is a common client complaint, but massage therapists often disregard the coccyx as a possible pain generator. This is due to a lack of biomechanical knowledge about the coccyx, as well as concerns about how to safely assess and treat this structure. When seated, the coccyx and bilateral ischial tuberosities form an elegant weight-bearing tripod.
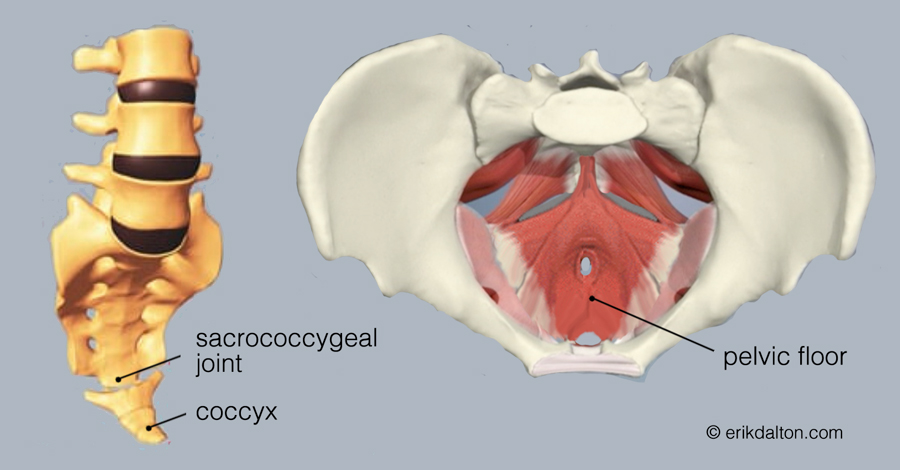
Although the coccyx bears minimal weight when sitting — about 10 percent like the fibula — it can be a major pain generator. Events such as childbirth or falling on the tailbone can lead to coccygeal pain, known as coccydynia. In most cases, the pain is caused by an unstable coccyx, resulting in chronic inflammation of the sacrococcygeal joint, along with protective guarding in associated muscles (Image 1).
Anatomical considerations
Many of us have been taught that the three or four bones of the coccyx fuse into one rigid segment by adulthood. However, several well-designed studies have shown there should be two or three movable parts within the coccyx that gently curve forward and slightly flex as we sit.1 In fact, the authors of two medical papers found that people with fused coccyges that were unable to flex upon sitting were more likely to experience tailbone pain than those with a normal coccyx.2,3 The primary conditions associated with coccyx pain in these studies were coccyges that were angled sharply forward (hooked coccyx) and bent more to one side.
Image 1. An inflamed coccyx may cause spasm in pelvic floor muscles
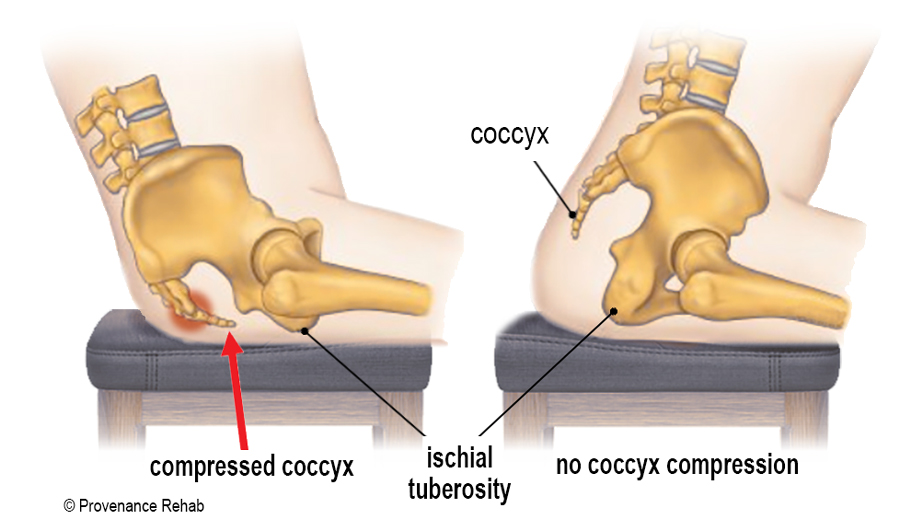
As for symptoms, the study participants reported dull, aching pain emanating from the gluteal cleft just superior to the anus and sometimes stabbing pain when rising from prolonged sitting. They also complained of localized pain after long periods of driving, biking, and sitting on hard surfaces, and many found that shifting weight from buttock to buttock temporarily relieved their symptoms. Because the coccyx bears more weight when a seated person leans back, we often see clients with coccyx pain flexing at the hips to shift more weight to their sitz bones (Image 2).
Image 2. Clients with coccyx pain may lean forward to relieve coccyx compression
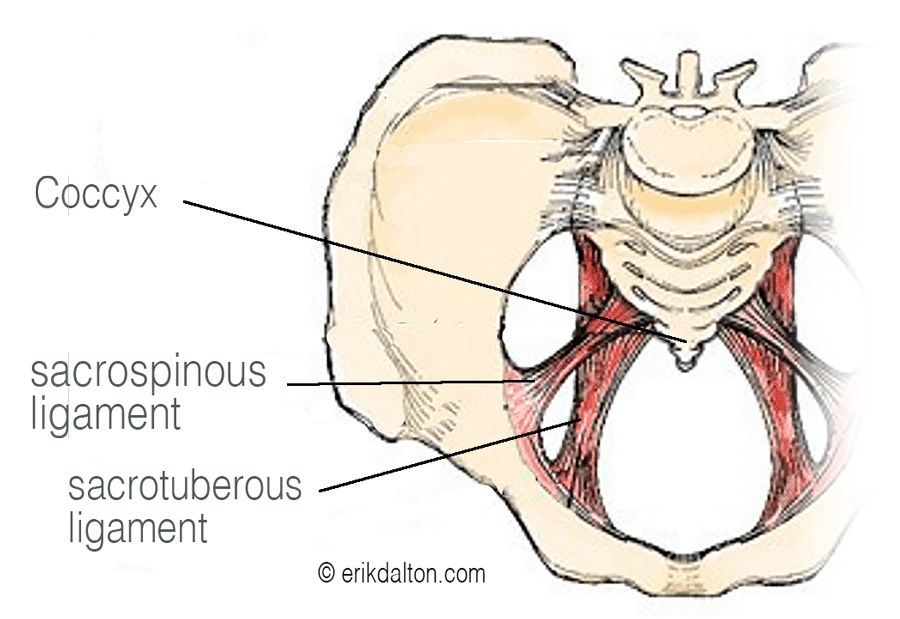
In humans, the coccyx serves important biomechanical functions and is an attachment site for various muscles, tendons, and ligaments. Muscles originating on the posterior coccyx include the gluteus maximus and strands of biceps femoris, which is often continuous with the sacrotuberous ligaments. Although multiple important ligaments attach to the coccyx, the ones I feel are most important for treating a hooked and sidebent coccyx are the sacrotuberous, sacrospinous, and lateral sacrococcygeal ligaments (Image 3 and 4).
Image 3. The sacrotuberous and sacrospinous ligaments
Image 4 . An injured sacrococcygeal ligament (SV) can drag the coccyx forward, fixate the joint, and impact pelvic floor function
Assessment and treatment
During the history intake for clients presenting with localized buttock pain, therapists can apply clinical reasoning to collect information by asking basic questions, such as:
How do you think your pain began?
Why do you think it continues to hurt?
What kind of movements trigger the pain?
When did you first notice the pain?
Where do you feel the discomfort, and can you reproduce the pain by pressing on a particular spot? Working through these questions in the intake interview not only helps pinpoint the injury site and possible tissues involved, but also reinforces that the client is being heard and that you will be working together as a team to help relieve their symptoms.
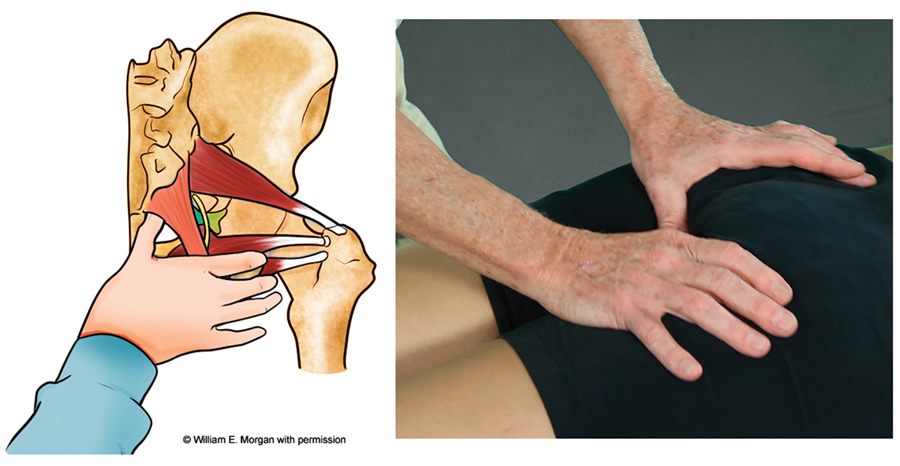
Massage therapy can be used as a conservative treatment for a coccyx injury by aiming to restore flexibility to surrounding buttock muscles. From there, the therapist can use ligaments as levers to help move the coccyx back to a more functional position. This can be done with the client prone or sidelying. In Image 5, I stand on the side toward which the coccyx is bent so I can hook my thumbs under the contralateral sacrotuberous and sacrospinous ligaments. The goal is to scoop up under the ligaments and gently traction the tissue posteriorly to reposition the hooked and sidebent sacrococcygeal joint. After holding for a period of 10-to-60 seconds the tissues surrounding the coccyx should begin to release. If you do not feel the tissue easing, a movement enhancer such as slow pelvic tilting or deep inhalation and exhalation often does the trick.
An important note to therapists treating coccyx dysfunction: Always ask the client’s permission to perform this technique due to possible physical and emotional hypersensitivity in the area, and work through clothing or draping to better allow the client to relax. In addition, before performing any type of coccyx work, take time to clearly explain what you’re doing and the desired outcome.
Image 5. The therapist can use ligaments as levers to help move the coccyx back to a more foundational position
References
Lirette, L.S., Chaiban, G., Tolba, R., & Eissa, H. (2014). Coccydynia: an overview of the anatomy, etiology, and treatment of coccyx pain. Ochsner Journal, 14(1), 84-87.
Postacchini, F., & Massobrio, M. (1983). Idiopathic coccygodynia. Analysis of fifty-one operative cases and a radiographic study of the normal coccyx. Journal of Bone and Joint Surgery, 65(8), 1116-1124.
Kim, N.H., & Suk, K.S. (1999). Clinical and radiological differences between traumatic and idiopathic coccygodynia. Yonsei Medical Journal, 40(3), 215-220.