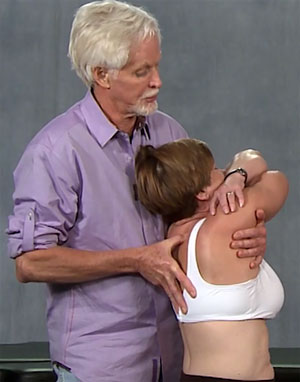
Brenda was referred to me for treatment of chronic (non-traumatic) head, neck, and thorax pain, exacerbated by more than two decades of job-related computer work. In the intake evaluation, Brenda was asked to assume her usual computer posture while I examined her cervical spine. With my left hand bracing her forehead, my right thumb and index finger began gently palpating tissues at the occipitoatlantal (O-A) joint. Right away, Brenda whispered, “That’s where my headaches begin.” Notice in the photo below how Brenda’s head is forced to cock back on the atlas to level her eyes. Some with this desktop posture experience neurovascular O-A compression, suboccipital spasm, t-spine rigidity, and, if the brain perceives threat… pain.

Notice how Brenda’s cocked head and jutted chin compresses the lower cervical facet joints creating protective guarding and an unsightly dowager’s hump. When asked to slowly forward-bend her neck, Brenda’s right T1 transverse process pushed back into my palpating thumb, indicating that the T1 facets were not opening on T2. In the early stages, this facet fixation probably didn’t excite enough mechanoreceptors to elicit a pain response, but prolonged t-spine rigidity combined with cervical nerve root stretching may have caused an inflammatory response that finally compelled the brain to elicit a pain response.
As Brenda’s normal movement patterns were altered by persistent pain, joint fixations, nerve entrapment and protective muscle guarding, new neuronal pathways were burned into her central nervous system. In Brenda’s case, the protective muscle guarding and t-spine immobility were treated using nerve and joint mobilization techniques such as the ones shown in the videos below. Once spinal rigidity and protective guarding were relieved, corrective exercises helped restore functional length/strength balance.
Lift thorax into extension to relieve t-spine compressive forces
- Client crosses arms across body and lifts elbows toward ceiling
- Therapist’s left arm comes under client’s folded arms, grasps her body, and extends his legs to lift client into extension
- Therapist’s right thumb contacts and pins dowager’s hump on client’s right while lifting and left rotating her torso searching for areas of restriction or tissue texture abnormality
- If resistance is palpated, client gently left rotates against therapist’s resistance to a count of 5 and relaxes and therapist brings her into her next restrictive barrier
- Repeat on both sides as needed
Chair stretch to help close fixated facets

- Client sits in chair and lowers her body so she can use the back of the chair as a fulcrum to place pressure on the dowager’s hump area
- Client places hands behind her neck, chin tucks, and reaches back with elbows to stretch front line and apply pressure to facets stuck in flexion
- Client rolls down the chair to help mobilize any vertebral segment that feel tight or sore
- Client repeats as necessary always making sure to keep the ribcage down