Many of your chronic pain clients may also be suffering emotional disorders such as anxiety, anger, depression, and poor coping skills (Fig. 1). Could you guess which ones are popping antidepressants and sleeping pills or various pain medications? Prolonged neck or back pain may disrupt normal sleep cycles, leading to central nervous system hyperexcitability, functional deficits, and physical deconditioning due to decreased physical activity and “fear of re-injury.

But many suffer CNS agitation in the absence of pain. For instance, during an Advanced Rolfing® class in the early 80s, Jan Sultan and Jim Asher (instructors) invited Boulder–area mothers with “special-needs” children to join us for a free manual therapy evaluation. This allowed students a chance to work with non-typical cases while gifting the children with some compassionate touch.
Early the first morning, a young Swedish lady arrived for her appointment with two sons, one seven and the other five. The eldest boy was calm and very well mannered, but Billy, the five year old, seemed dissociated and hyper-stimulated, i.e., wired for sound. Although Billy did not display anger, it just seemed he was not “happy in his skin.” He couldn’t focus long enough to look you in the eye, and his mother, with all her good intentions, had no clue how to handle this child, and neither did the teachers at his pre-school.
When asked about previous medical conditions or accidents, the distressed mother related a story of how her son took a bad fall on his butt during a skateboarding incident a year earlier. According to film studies by two physicians, the boy suffered no serious injuries other than a bruised hip and a scraped elbow. Within days however, the family began noticing personality changes in Billy…they summed it up this way “Billy began living in his own world.”
 Jim Asher asked the class to pay attention to the boy’s bug-eyed and glazed look as he continuously surveyed the room. It was obvious that something had turned the volume up in this young man’s nervous system….but what? I think most of the students were expecting the two veteran instructors to “Tag-Team” Billy on the therapy table. Instead, Jan Sultan crawled down on the floor and began playing and mimicking Billy’s movements. Within 10 minutes or so of light wrestling, Billy was squirming a bit less, which allowed Jan the opportunity to do some palpation and assessment.
Jim Asher asked the class to pay attention to the boy’s bug-eyed and glazed look as he continuously surveyed the room. It was obvious that something had turned the volume up in this young man’s nervous system….but what? I think most of the students were expecting the two veteran instructors to “Tag-Team” Billy on the therapy table. Instead, Jan Sultan crawled down on the floor and began playing and mimicking Billy’s movements. Within 10 minutes or so of light wrestling, Billy was squirming a bit less, which allowed Jan the opportunity to do some palpation and assessment.
As Jan’s experienced hands worked through Billy’s musculoligamentous pelvis, he suddenly hit a spot on the coccyx that sent the boy reeling and crawling to his mom. Apparently, this came as no surprise to mom. She was aware that he ‘favored’ that area, and that he avoided sitting as much as possible, but the docs assured her everything ‘down there’ was OK!
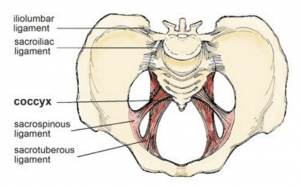
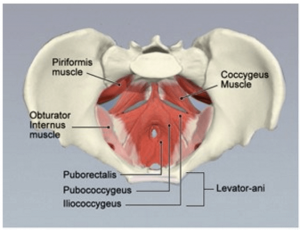
Jim Asher playfully held him, Jan was able to palpate a severely ‘hooked’ and sidebent coccyx (Fig. 2). Most of the following images can be found in Dalton Technique Tour course under “Coccyx Work”. The small class of Rolfing students watched intently as Jan explained how he was loosening the sacrotuberous, sacrospinous and sacrococcygeal ligaments to create space for the coccyx to move posteriorly into a more neutral position (Fig. 3). Unfortunately, one of the ‘keys’ to helping the coccyx move back after ligament loosening is to have the client perform some type of posterior chain hyperextension maneuver, i.e., cobra. As the L5 facet joints glide down on top of the S1 facets, they push both sacral bases anteriorly (sacral nutation) causing the coccyx to glide posteriorly and sometimes ‘unhook’.

It is also helpful to teach coccydynia sufferers a ‘reverse kegel’ maneuver that fires the pelvic floor muscles which pushes on the ligamentous web encasing the coccyx (Fig. 4).
Well, that just wasn’t possible with Billy, so Jan went back to work this time using his little finger to dig under the edge of the sidebent coccyx attempting to release the tissue binding the hooked joint. Finally, to the surprise of everyone in the room…it happened. The crooked sacrococcygeal joint suddenly gave way and reluctantly slid back where it was before the fall.
A sound of silence filled the classroom, as we observed Billy settling back into his body; beginning to look around as if he’d not been there before. Apparently, Jan’s coccyx work down-regulated Billy’s fight-or-fight response to a point where he was able to fix his gaze on a still object and connect with it. His mother wept in disbelief and the class was speechless. My only thought was, “I wish I had this on film.”
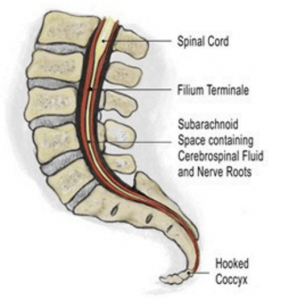
So what was the etiology of the injury and why did the coccyx work calm Billy’s nervous system. No one is sure, but some believe that when a coccyx hooks, it tugs on the dural membrane via the filum terminale, a long, slender connective tissue strand that terminates at the end of the spinal cord (Fig. 5). This, in turn, is believed to cause dural drag, loss of cerebrospinal fluid flow, and resultant CNS irritation. Difficulty sitting for any length of time, problems with sex, urination, PMS, bed wetting, digestion and extreme sensitivity to light also raise red warning flags of possible coccyx dysfunction, i.e. coccydynia. A modified version of Rolf’s coccyx technique is demonstrated in the video below.
NOTE: Always ask the client’s permission when performing this technique due to possible physical and emotional hypersensitivity in the area. Before performing any type of coccyx work, take time to clearly explain what you’re doing and the desired outcome.