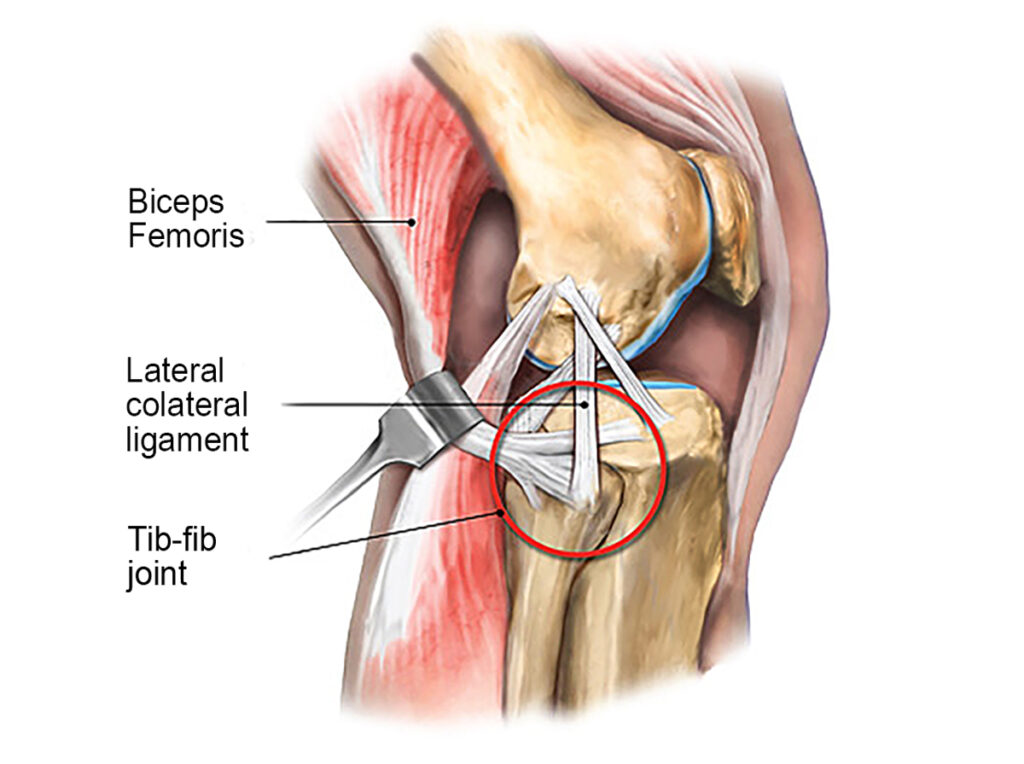
One of the primary functions of the tib-fib synovial joint is to help dissipate lower leg torsional stresses during gait. When the knee is extended, the biceps femoris, popliteus, and lateral collateral ligaments provide good joint stability, but with the knee flexed, these connective tissues lose much of their supportive capability. That’s one reason tib-fib injuries are most often seen in sports that involve twisting forces around the knee and ankle, such as football, wrestling, soccer, judo, gymnastics, long jumping, and skiing.
In my non-athletic clients, tib-fib problems typically arise from overuse injuries on jobs that require repetitive activities. Clinically, I’ve found many clients presenting with lateral tib-fib pain from overuse also have an underlying body structure deficit, such as overpronated feet and valgus knees. In these cases, forces accumulate that cannot be properly dissipated or, worse yet, may be misdirected into areas not intended to handle the load, as we will see in the case study presented later in this article.
Image 1. Tib-Fib joint with stabilizing muscles and ligaments
Common signs and symptoms of tib-fib dysfunction:
Pain with one-legged weight bearing
Outer knee pain aggravated by direct pressure to the fibular head
Limited knee extension
Crepitus (grinding) during knee movement
Visible deformity
Ankle movements that provoke lateral knee pain
Palpation and Assessment
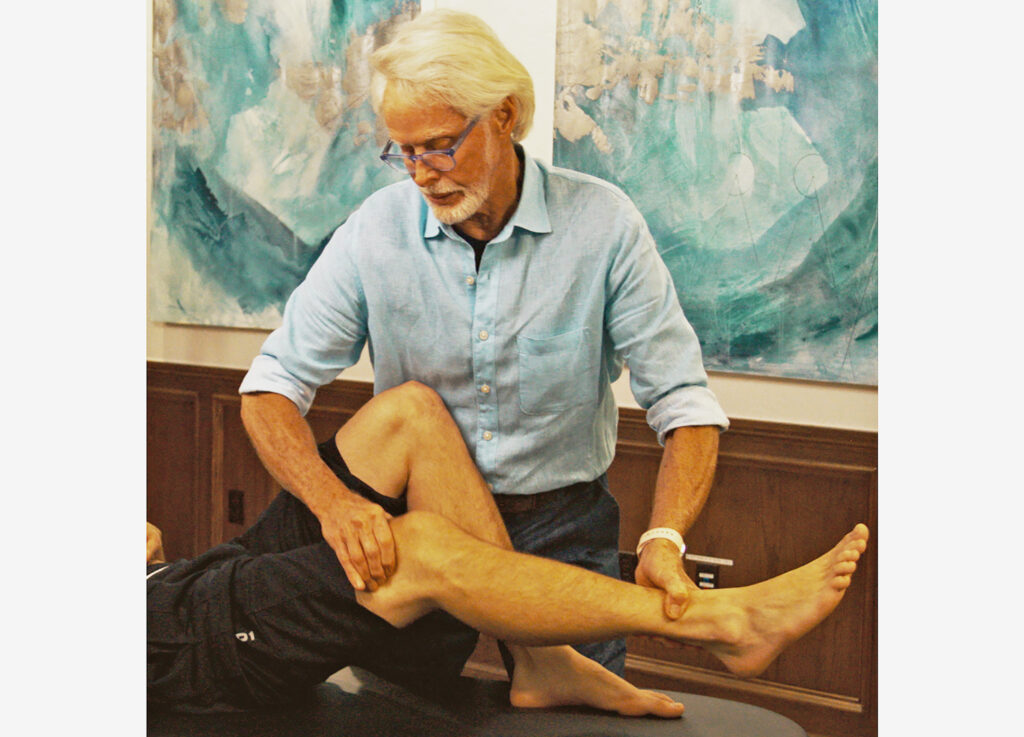
Yale University researcher Dr. John Ogden was the first to conduct studies evaluating the anteroposterior (A-P) motion of the proximal fibula and correlating it with positional changes of the knee.1 He found that when the knee flexes, the proximal fibular head moves anteriorly, and during knee extension, the fibula translates posteriorly (approximately one centimeter in both directions). In Image 2. , I demonstrate an assessment version of Ogden’s A-P glide on my client Keith’s right knee.
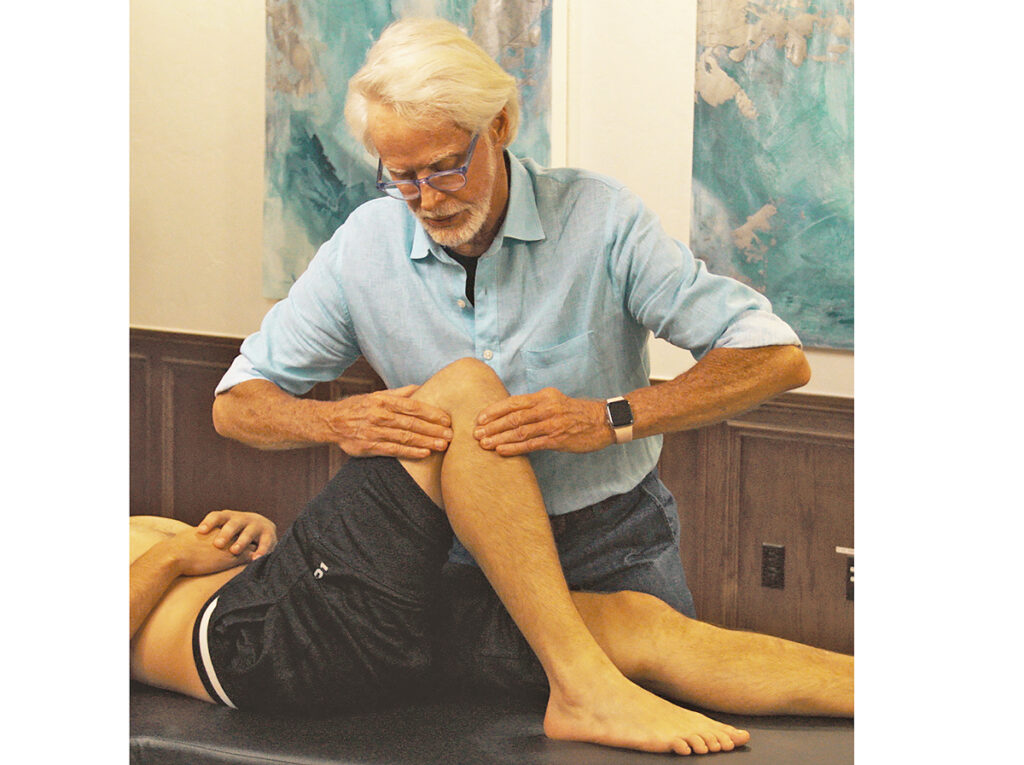
With index finger and thumb, I first locate a medium-sized bump on his lateral leg about two inches inferior to the knee. To confirm I’m palpating the proximal fibular head, I simply flex Keith’s knee to 90 degrees, locate the biceps femoris hamstring tendon just behind the lateral knee, and apply resistance as he attempts knee flexion (Image 3. ). If I feel the biceps femoris tendon tighten, I know I’m in the right spot.
Image 3. To confirm that I’ve located the client’s fibular head, I palpate the biceps femoris tendon behind the lateral knee and apply resistance as Keith attempts knee flexion
Image 2. With client’s knee flexed and foot resting on therapy table, my fingers palpate the fibular head and begin translating forward and back assessing for lack of joint play
Keith’s Case Study
When assessing Keith’s A-P glide, I noticed a restriction to anterior translation of fibula on tibia accompanied by tenderness and a slight grinding noise. I recalled that during Keith’s history intake he described a pretty significant inversion ankle sprain and hamstring contusion experienced during a judo fall that left him with a temporary limp, intermittent lateral knee pain, and lower leg numbness.
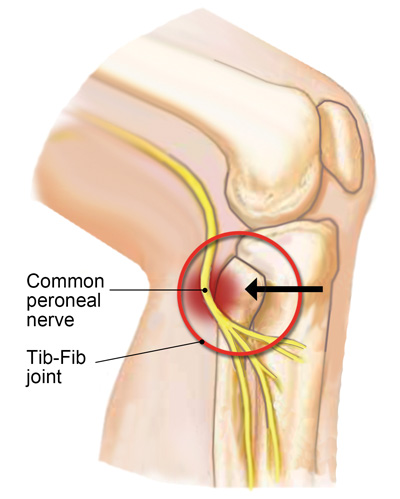
Image 4. Common peroneal nerve impingement due to a posteriorly fixated fibular head
Using a clinical reasoning approach, I intuited that his posteriorly fixated fibular head might have resulted from shortening of the biceps femoris muscle following his traumatic judo injury. Further, I reasoned that Keith’s intermittent lower leg paresthesia might have been triggered by common peroneal nerve irritation due to his posteriorly fixated fibular head (Image 4. ). To validate my findings, I asked Keith to stand on the affected leg and bend his knee to 30 degrees. This maneuver did reproduce Keith’s knee and leg symptoms and is a very good confirmation test for tib-fib joint dysfunction.
Image 5. I apply a basic hamstring stretching technique to address the client’s chronic hamstring injury and to relieve posterior drag of the biceps femoris tendon on his fibula
In Image 5. , I apply a graded exposure hamstring stretching technique (using movement enhancers) to help relieve posterior drag of the biceps tendon from Keith’s fibular. This stretching maneuver is great for those biceps femoris muscle injuries where there is accumulated scar tissue and the brain is protectively guarding the area. Once I was able to improve Keith’s hamstring flexibility, I chose a simple myoskeletal technique to help move the fibula forward on the tibia, then retested for improved tib-fib mobility (Image 6. ).
Image 6. My middle and ring fingers hook under the client’s fibular head. As my right hand flexes and abducts the client’s knee, my fingers pull anteriorly on the fibula to help restore Tib-Fib joint play
Summary
If you have a client with knee pain that fits some of the patterns outlined above, the tib-fib may be involved. In such cases, the first order of business is to determine the type and degree of tissue damage based on history, assessment, and clinical reasoning. Left untreated, tib-fib fixations can cause long-term difficulties including pain, gait disturbance, and inferior sports performance. Hopefully, a better understanding of this often-neglected joint leads to less clinical error and improved client outcomes.
References
1. Ogden, J.A. (1974). Subluxation and dislocation of the proximal tibiofibular joint. Journal of Bone & Joint Surgery, 56(1), 145-154.