Theory of shoulder girdle function
The shoulder girdle functions to position the hand, provides stability for hand use, lifts, pushes, elevates the body, assists with forced inspiration and expiration, and even weight bearing as in crutch-walking. The hand performs a significant range of functions. It is an organ of touch, an extension to the brain that provides information to the visual system about the environment, and it is an important organ for expression and nonverbal communication. The hand can grasp with forces exceeding 100 pounds as well as hold and manipulate a delicate thread. Unfortunately, optimal hand functioning is often jeopardized by problems occurring in the shoulder girdle, elbow and wrist.
Most Myoskeletal seminars begin with assessment and treatment techniques aimed at restoring length-tension balance between tonic and phasic (tight-weak) muscle groups of the torso. Typical imbalances between these two muscular systems lead to aberrant strain patterns such as Vladimir Janda’s upper and lower crossed syndromes and scoliotic (torsional) asymmetries. Tension, trauma, and repetitive movements combined with gravitational exposure alter the position and function of associated joints. Mobilizing joints through muscle manipulation is at the heart of the myoskeletal method. Therefore, soft tissue maneuvers have been developed to release osseous fixations and help create joint-play in all the body’s synovial joints.
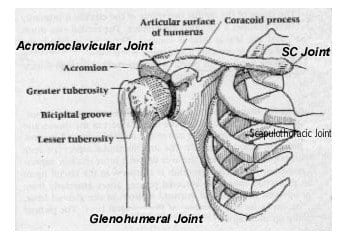
Those of you who have taken my Advanced Shoulder, Arm & Hand workshop or viewed Volume III, Myoskeletal Techniques videos are aware that the assessment and treatment order is reversed when dealing with loss of range of motion and stability in the upper extremities. In my personal experience, I have found that many painful shoulder, arm and hand conditions do not fully recover until each articulating joint surface (sternoclavicular, acromioclavicular, glenohumeral, radioulnar, and carpals) is addressed in a precise order. Most massage therapists are unaware of the precise range of motion options that must be present in each joint so fluid movement can travel smoothly down the shoulder girdle’s kinetic chain and into the hand. When active stretching techniques are properly applied to a joint and its associated soft tissues via muscle energy (contract-relax) techniques, many cases of tendinitis, nerve impingement and referred pain suddenly disappear.
Active movement psychologically reinforces to a client that she can move the arm through a greater range of motion. Physiologically, active movement assists the healing collagen tissue to align itself along normal stress lines and aids in restoration of normal strength. Active movement also nourishes articular cartilage and enhances its repair. Active exercises, such as scapular plane elevation and external rotation, facilitate muscular strength and endurance while augmenting the joint mobilization intervention with regular stretching. This is important because musculotendinous structures return to their resting length within a few minutes following active isolated stretching.
For example, when testing the sternoclavicular joint, the medial heads of the clavicle must drop down during shoulder elevation and must move posteriorly during horizontal extension of the arms. The acromioclavicular joint has three motions that can become dysfunctional, the glenohumeral ten, the elbow three, and so on down the arm. When performing upper extremity work, I first take my clients through a systematic 15 minute mobilization routine beginning with the sternoclavicular (SC) joint, and proceed with assessment and correction of all bony articulations in the shoulder, elbow, wrist, and hand. Any remaining soft tissue restrictions and/or pain sites are then evaluated using the acronym ART:
- Asymmetry
- Restriction of Motion
- Tissue Texture Abnormalities.
Mobilization techniques apply distraction, compression, rotation, and/or translation forces to bones to restore normal accessory joint mobility. Continual reevaluation of motion progression is valuable to provide clients with short- and long-term goals. This also gives the clinician feedback about compliance with the home exercise programs which includes Thera Band® strengthening tools and specific stretching modalities.
Pelvic & Trunk Stabilization
Of course, pelvic and trunk alignment and stabilization routines as presented in Myoskeletal Techniques Volumes I and II must precede any upper extremity work. This is obvious to most structural integrators and sports therapists. During a tennis serve for example, the power generated by the shoulder must follow a kinetic chain beginning with power produced by the legs, trunk and back. Since the muscle mass of the shoulder is relatively small, if inadequate momentum is generated by the preceding links in the kinetic chain, the shoulder has to play ‘catch-up’ and generate power rather than acting as a force regulator. Improving muscle/joint function in the server’s legs, lumbars and trunk stabilizers, allows reduction of the incidence of rotator-cuff injuries during the tennis player’s serve. Biomechanical analysis of specific joints is not difficult and can help rule out suspected soft tissue injuries. In skilled hands, joint mobilization through assisted stretching is a crucial and effective element in injury prevention.
Summary
The reflexogenic relationship of muscles and joints is at the heart of the Myoskeletal Method. Any alteration of joint function influences muscular function, thus producing a self-sustaining chain reaction. To understand the fine control of motion, the separate activity of individual muscles is not as important as their coordinated activity within the different movement patterns. The proper understanding of this concept appears as the best basis for rational treatment and good long-term therapeutic results in the general population, along with clients presenting with functional joint problems.
On sale this week only!
Save 25% off the Upper Body Course!

NEW! Enhanced video USB format!!!
Learn unique approaches to work with the shoulder girdle, arms, neck, and torso, this course will prepare you to relieve painful myoskeletal issues in the upper body. Through video demos and animation, you’ll learn to identify several compensatory movement patterns and their associated reflexogenic pain. With this understanding of where the true source of problems arise, you’ll be able to develop highly effective treatment protocols and deliver lasting results. This course provides you with the skills you need to confidently relieve pain issues in the upper body. (20 CE)
Bonus: When you order the Home Study version, get the eLearning course and and an additional 2CE Ethics eCourse for free!
Save 25% off the Upper Body Course this week only. Offer expires Sunday, March 1st. Click the button below for more information and to purchase the course for CE hours and a certificate of completion to display in your office.







