As published in Massage & Bodywork Magazine
Addressing Joint Misalignment
A joint’s normal range of motion is defined by the connective tissue that binds it. The muscles, tendons and fascia that cross a joint dictate approximately 80% of its stability with less than 20% entrusted to the ligaments. Ideal body balance requires some muscles to act as stabilizers and others to act as mobilizers, depending on joint position and movement required for the particular task. A perfect balance of mobilizers and stabilizers results in optimal alignment, or joint centration.
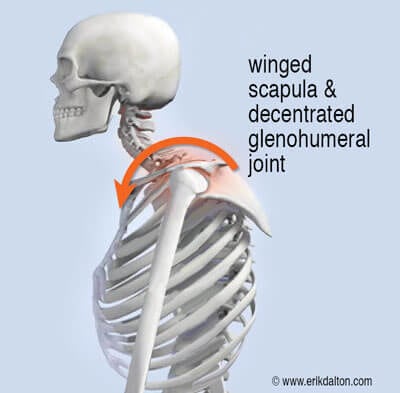
Think of joint centration like the wheel on a car. If the center of rotation is aligned with the center of the hub, it will deliver the most efficient performance. Conversely, when this neutral position becomes misaligned, the wheel spins incorrectly and can result in future mechanical problems. We commonly see this in upper crossed syndrome (UCS) postures where slumped shoulders and a head-forward carriage lead to scapular winging and decentration of the glenohumeral joint (GHJ) (Img. 1).
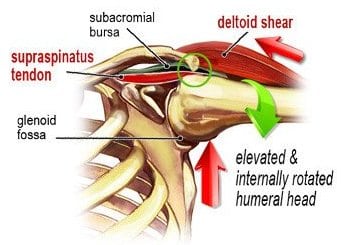
A key function of the cuff muscles is to maintain the head of the humerus centrated within the glenoid cavity (concavity compression), and at the same time, impose an inferiorly directed force to the humeral head. In those with rounded shoulder postures, the glenoid fossa’s mechanical axis of rotation is altered, causing the brain to activate muscles that are typically at rest, such as upper trapezius, levator scapula, pectoralis minor and deltoids. Postural overdevelopment of these muscles undermines rotator cuff stability, causing a ‘deltoid shear’ that elevates and crams the humeral head into the top part of the glenoid fossa (Img. 2). As the person abducts the arm to 90°, the supraspinatus tendon abuts the acromion, causing micro-fraying, fibrosis, and possible tendinosis.
Until upper crossed postures and core instability issues are addressed, it does little good to address the deltoid hypertonicity, or offer home retraining exercises to strengthen the rotator cuff. In the 2014 Stanford Sports Medicine Center debate, Gray Cook, PT, stated: “When I say ‘mobility first’, it is not simply an invitation to stretch or mobilize. You must first explain why mobility is limited or compromised. Look closely and you will often find that a tight muscle is limiting a movement pattern where motor control or stability is poor.” Stewart McGill, PhD, countered, “The spine must first be stable before movements and forces are produced to enhance performance.”
Of course, both men are right. Ground up core stability is paramount for optimal joint centration and shoulder function. The saying, “You can’t shoot a cannon from a canoe,” sums up the importance of spinal stability in all upper (and lower) extremity movements. As stated in my Massage & Bodywork column “Finding the Weak Key Link,” the thoracic spine and ribs must be mobile and the scapular muscles stable. In today’s desk-occupied, sedentary lifestyle, function is often reversed as the t-spine stiffens and the scapulae flare, leaving an unstable anchor for the GHJ. The decentrated joint predisposes the rotator cuff to injury, particularly in those who participate in activities requiring the use of overhead arm positions such as painters, tennis players and gym-junkies.
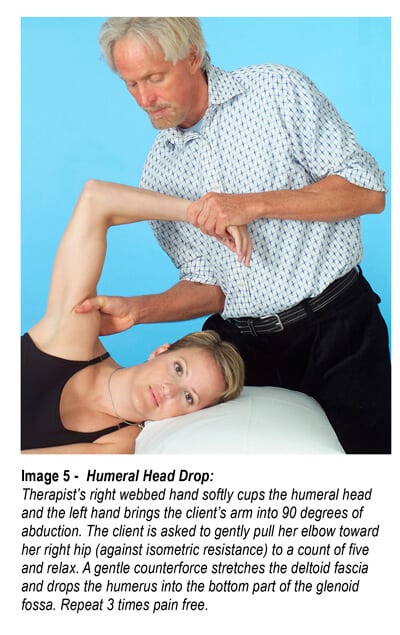
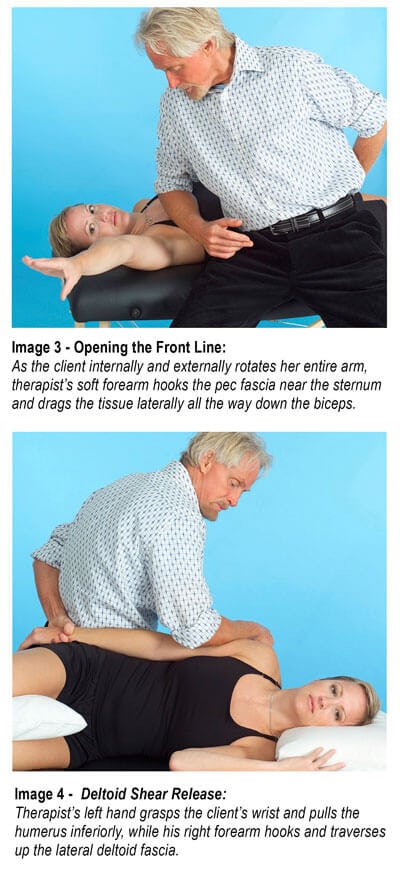
Img. 3, Img. 4 and Img. 5, are examples of techniques I’ve found helpful in addressing upper-crossed syndromes, deltoid shears, and rotator cuff injuries. Once proper glenohumeral mobility is restored, home retraining advice should include exercises for core stability, scapular stabilization, and rotator cuff strengthening.
Remember: mobility first. Refrain from advising muscle-strengthening exercises for joints that are not moving freely. This can lead to cartilage degradation and ultimately capsulitis or osteoarthritis. When massage and movement therapists successfully restore length-strength myoskeletal balance, tissue lubrication improves and the transmission of nerve impulses becomes more efficient. Better proprioceptive neural feedback enhances motor control and reduces injury in clients with the “wobbly wheel” syndrome.