Introduction
Manual therapists often spend hours working with the spine, hips, shoulders, and neck, yet the abdomen is easy to avoid. It can feel personal, vulnerable, or outside the familiar territory of musculoskeletal work. But the abdomen is an important link to posture, breathing, spinal motion, pelvic support, and the nervous system.
Thoughtful abdominal work can provide gentle mechanical input to the diaphragm, abdominal wall, pelvic bowl, and colon pathways. It can help reduce guarding, improve comfort with abdominal breathing, encourage a sense of space through the trunk, and support the client’s awareness of this often-neglected region.
Research on abdominal massage is still developing, but there is some evidence that abdominal massage may help with symptoms of functional constipation. We want to frame this work as supportive, not curative. It may be helpful for comfort, motility awareness, breathing, and tissue mobility, but it is not a replacement for medical care.
Practice along with the video demonstration until you know the sequence well. Always explain the work clearly, receive specific consent, use appropriate draping, and remind the client they can ask you to stop or change pressure at any time. Avoid deep abdominal work with unexplained abdominal pain, fever, active infection, nausea, suspected hernia, and pregnancy complications. Repeat these techniques on both sides of the body.
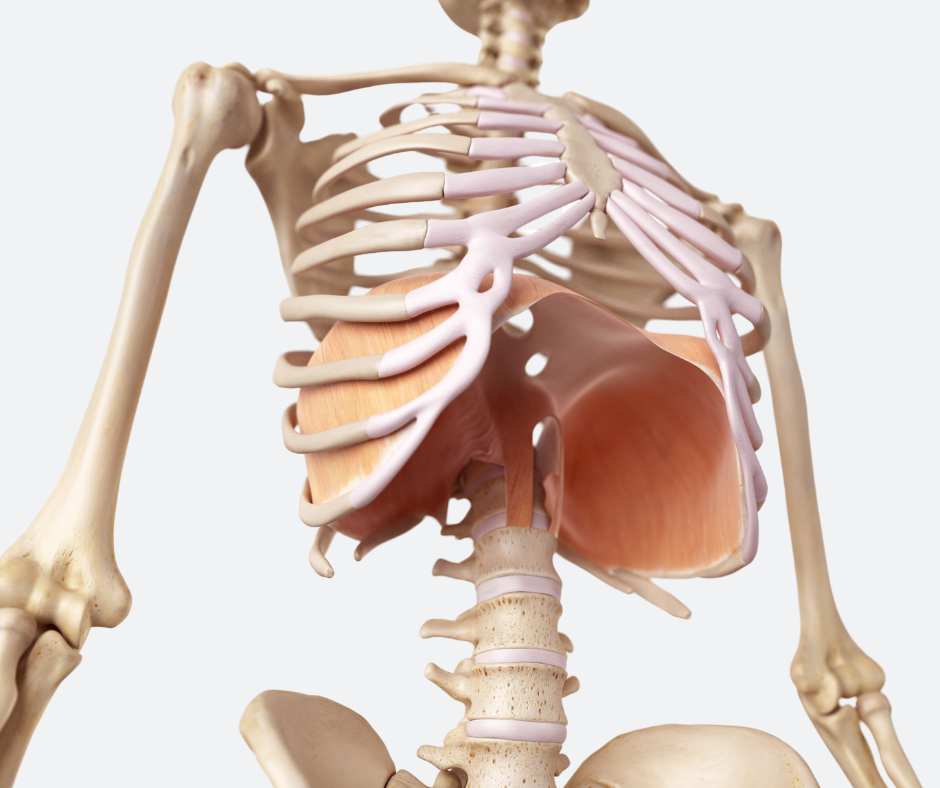
Diaphragm Mobilization
Begin with the client supine. Stand beside the table and soften the web of your hand so it can make broad, comfortable contact along the lower costal cage. Rather than poking under the ribs, widen your hand and let your body weight sink gently into the tissue.
The diaphragm descends during inhalation and rises during exhalation. Many clients with abdominal guarding, rib restriction, or shallow breathing have difficulty allowing the lower ribs and belly to expand. In this technique, you provide gentle resistance at the costal margin while the client breathes into the lower belly.
Ask the client to take a slow, full inhalation toward the lower abdomen. As they inhale, maintain a soft, steady resistance so the diaphragm and lower rib cage have to move against your hand. Then ask the client to hold the breath briefly while you gently pump the tissue upward toward the rib cage. The movement should feel like a rhythmic lift, not a thrust or forceful compression.
The intention is to improve diaphragmatic excursion, reduce protective tone around the lower ribs, and help the client reconnect breath with abdominal movement. Keep the pressure comfortable and avoid creating the need for the client to brace or guard.
Lower Abdominal and Ascending Colon Mobilization
Next, move to the lower right abdomen near the inside of the ilium. Cup the ilium with your hand so the heel of your hand and palm fit comfortably into the lower abdominal wall. Use body weight rather than arm strength, and sink in slowly.
This area corresponds generally with the beginning of the ascending colon and the lower abdominal tissues that blend into the iliac fascia, obliques, and pelvic bowl. The goal is not to “push the colon” or force digestive movement. The goal is to introduce broad, sustained contact while the client adds gentle pelvic motion.
Ask the client to perform slow pelvic tilts. As they rock the pelvis, maintain steady contact and allow the tissues to move beneath your hand. This adds active movement through the abdominal wall, pelvis, and lumbar region while your hand provides a stable point of reference.
This technique can be useful when the lower abdomen feels guarded, compressed, or disconnected from pelvic movement. It also gives the client a simple way to feel how abdominal tone and pelvic motion influence one another.
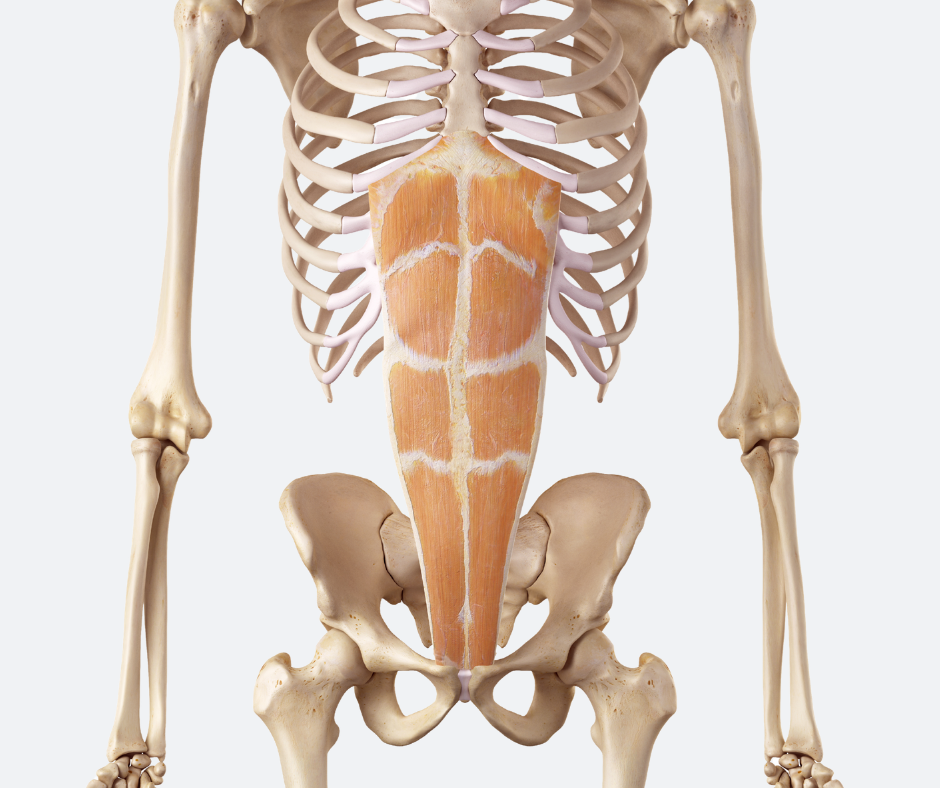
Rectus Abdominis Midline Support
The rectus abdominis runs vertically on either side of the linea alba. During pregnancy, the rectus muscles may separate as the abdominal wall stretches. This condition is known as diastasis recti. It can leave the client with a visible abdominal bulge, reduced trunk support, or a sense that the abdominal wall does not generate pressure well. Specific rehabilitative exercise is usually central to recovery, and more significant cases may need medical or physical therapy support.
Manual work should not be described as closing or repairing a diastasis. Instead, think of this technique as helping the client sense the lateral borders of the rectus abdominis and encouraging the abdominal wall toward midline awareness.
To locate the lateral border of the rectus, place your fingers along the side of the muscle and ask the client to gently lift their head. As the rectus contracts, you can feel its edge become more defined. Ask the client to lower the head, then use your fingers to gently hook the lateral edge of the rectus and scoop the tissue toward the midline at a slight oblique angle.
Avoid digging, pinching, or pulling directly into the linea alba. This work should be slow, precise, and comfortable. The client’s breath should remain easy. The intention is to improve proprioception, abdominal wall organization, and a sense of support through the front body.
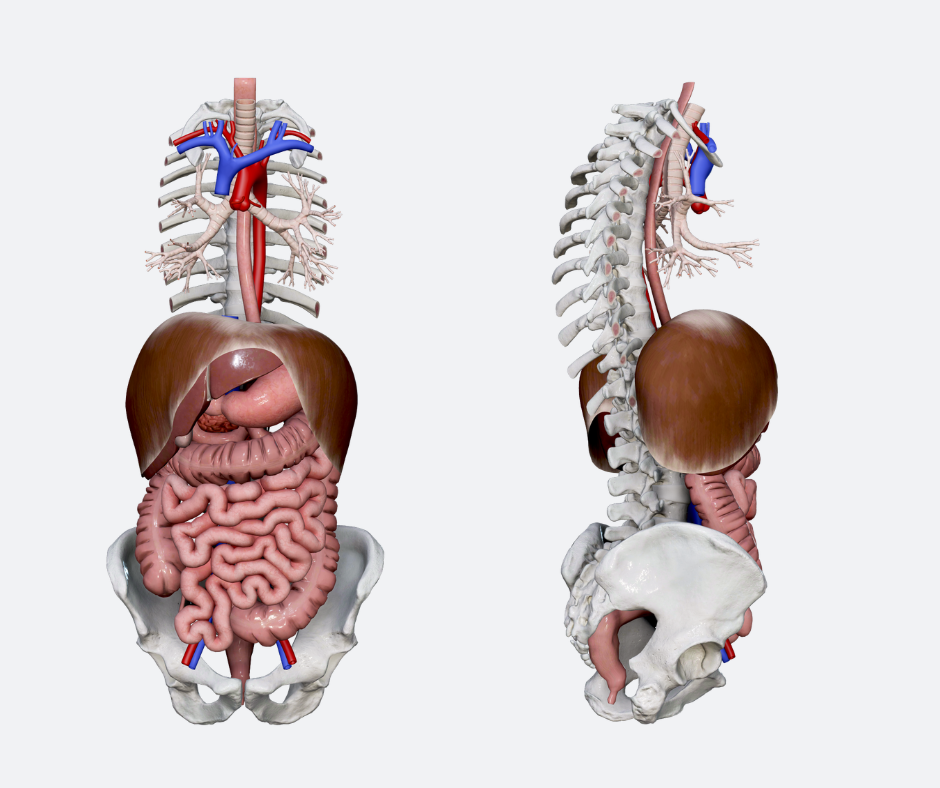
Ileocecal Region Work
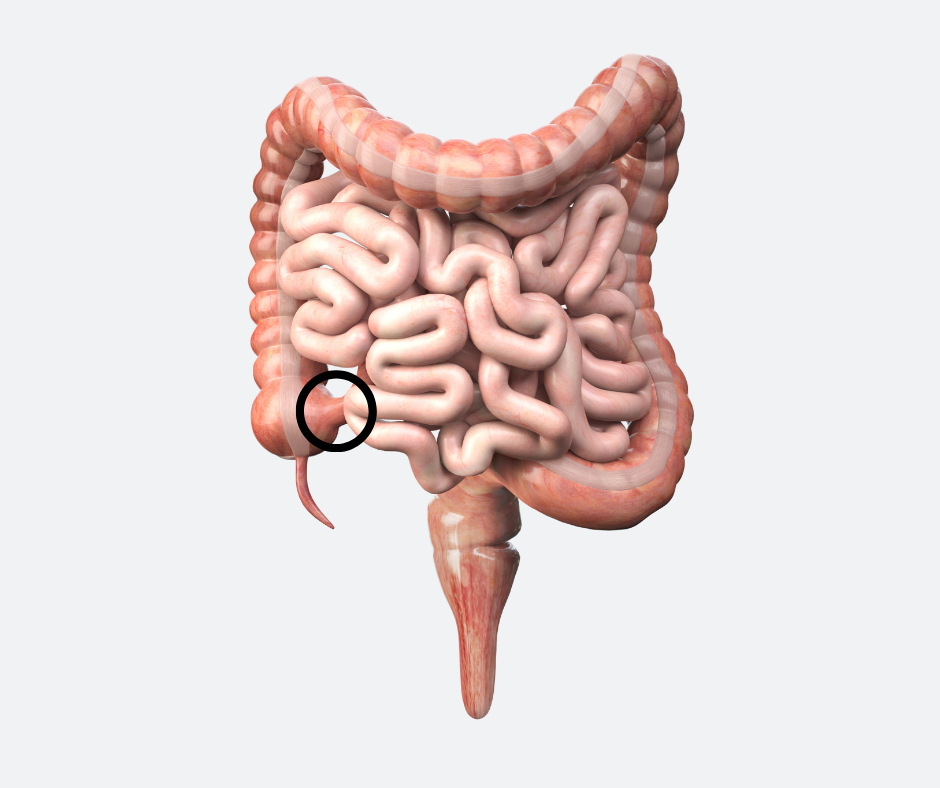
The ileocecal valve sits between the small intestine and large intestine (circled on the diagram above). It helps regulate movement from the ileum into the cecum. Dysfunction in this region is sometimes discussed in relation to bloating or small intestinal bacterial overgrowth, but massage therapists should be careful with this language. SIBO is a medical condition involving excess bacteria in the small intestine and requires medical diagnosis and treatment.
There is research suggesting that low ileocecal junction pressure may be associated with SIBO, but manual therapy should not be presented as a way to diagnose, open, close, or correct the valve.
To locate the general ileocecal region, place one finger on the right ASIS and another at the belly button. The region halfway between those points approximates the area often used for ileocecal contact. Use two or three soft fingers and apply gentle circular movement. The transcript describes counterclockwise rotation, but the most important principles are comfort, slowness, and client feedback.
This area can be tender. Stay light. If the client experiences sharp pain, nausea, anxiety, guarding, or a sense that the contact is too invasive, stop or move away from the area.
Lower Abdominal and Pelvic Bowl Lift
Gravity, posture, breath-holding, pregnancy, surgery, and chronic guarding can all influence the way the lower abdomen and pelvic floor feel. Many clients describe heaviness, gripping, or compression in the lower belly. Manual work in this region must be handled with extra attention to consent, clarity, and boundaries.
Begin by asking the client to place their fingers on their own pubic bone so they understand the landmark. Explain that your contact will be just above the superior border of the pubic bone, not on sensitive tissue. Ask permission before placing your hand.
Once permission is given, place your hand just superior to the pubic bone. Let your body weight sink slowly toward the table. Do not slide immediately. First, wait for the tissue to soften around the contact. This should not be painful.
Once you have a comfortable tissue hook, slowly draw the lower abdominal tissue headward. Ask the client to perform gentle pelvic tilts as you maintain the lift. Their movement creates a mild activating force through the lower abdomen and pelvis while your hand encourages the tissues away from a compressed, downward pattern.
This technique should not be presented as lifting organs, treating prolapse, or correcting pelvic floor dysfunction. Pelvic organ prolapse, bladder symptoms, pelvic pain, and interstitial cystitis require appropriate medical or pelvic health referral. Interstitial cystitis, also called bladder pain syndrome, is a chronic condition that causes painful urinary symptoms. It is not the same thing as a bacterial bladder infection.

Side-Lying Colon Mobilization
With the client lying on their side, stand behind them with your hip gently braced near their pelvis or buttocks for stability. Keep your arms extended and use broad, comfortable contact through the side of the abdomen. From here, gently drag the abdominal tissue toward you.
On the client’s left side, this contact follows the general pathway of the descending colon. On the client’s right side, it follows the general pathway of the ascending colon. The transcript mentions the descending colon as an area where stagnation may occur. For accuracy, avoid linking this directly to cancer. Colon cancer can occur in different regions of the colon, and while left-sided colon cancer includes the descending and sigmoid colon and is more common than right-sided colon cancer, massage does not prevent or treat cancer.
A safer way to frame this technique is that it introduces broad, supportive movement to the lateral abdominal wall and colon pathway. It may feel relieving for clients who experience abdominal tightness, trunk compression, or restricted breathing through the side body.
For pregnant clients, keep the pressure gentle, avoid deep abdominal compression, and work only within your training and scope of practice. This is especially important in high-risk pregnancies or when the client has pain, bleeding, preeclampsia, placental concerns, or other complications.
Bringing the Routine Together
This short belly work routine can be performed in a few minutes, but the quality of the contact matters more than the speed. Move slowly. Use broad contact. Watch the client’s breath, face, abdominal tone, and nervous system response. If the client braces, holds their breath, or becomes uncomfortable, lighten the pressure or pause. Repeat these techniques on both sides of the body.
Performed well, belly work helps bring the abdomen back into the conversation. It reminds us that the trunk is not just a spine with muscles attached. It is a pressure system, a breathing system, a digestive space, and a deeply responsive region of the nervous system.