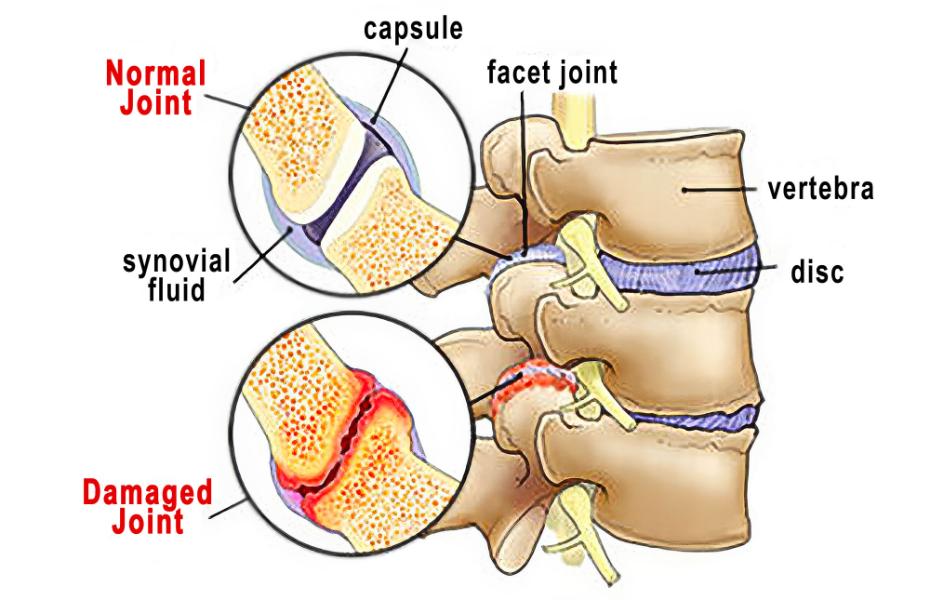
Many clients who come in with “nonspecific” low back pain may actually be experiencing mechanical stress in the zygapophyseal joints, also known as facet joints or Z-joints—small, paired articulations on the back of the vertebrae that guide spinal motion and share load with the intervertebral discs.
These joints are lined with cartilage, enclosed in a synovial capsule, and lubricated with fluid to allow smooth gliding between vertebrae. When healthy, Z-joints permit controlled motion, especially flexion, extension, and sidebending, while preventing excessive rotation that could damage the discs.
Unfortunately, wear and tear over time can compromise this elegant system.
Anatomy of the Z-Joints
Each lumbar vertebra connects with the one above and below through two Z-joints. Together with the intervertebral disc, they form a three-joint complex that balances mobility and stability.
- Structure: The articular surfaces are covered with hyaline cartilage and enclosed by a capsule rich in sensory nerves.
- Function: They bear roughly 20–25% of compressive load during extension and up to 50% during rotation (Adams & Dolan, 2005).
- Innervation: The medial branches of the dorsal rami transmit sensory information, explaining why inflammation here can cause sharp, localized pain near the spine.
Over time, repetitive strain, poor posture, injury, or degenerative changes can alter how these joints align and move—leading to inflammation, fibrosis, and bone spur formation.
How Z-Joint Dysfunction Develops
When cartilage thins and the capsule becomes lax or inflamed, motion becomes restricted and uneven. The resulting micro-instability leads to:
- Increased friction between articular surfaces
- Joint capsule irritation
- Chemical sensitization of the medial branch nerves
This chemical irritation can bombard the spinal cord with nociceptive signals, triggering muscle guarding and stiffness. In other words, the nervous system starts to “lock down” movement in an effort to protect the spine, ironically perpetuating the pain cycle.
Common contributors include:
- Repetitive bending or twisting
- Prolonged sitting or hyperlordosis
- Obesity or deconditioning
- Postural asymmetries or pelvic torsion