Acknowledging the A/C
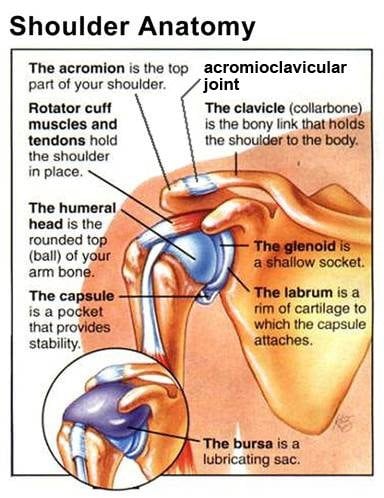
The Acromioclavicular or A/C joint sits on the point of the shoulder lateral to the sternoclavicular and proximal to the glenohumeral. This oft-overlooked bony articulation receives little respect from most manual therapists…a regrettable omission, indeed. Both the A/C and S/C joints play vital roles in the biomechanics of throwing and other upper-limb activities. A/C joint injuries typically occur from falling directly on the point of the shoulder. In competitive sporting events a direct clash of shoulders between players often displaces or completely subluxes this joint. Some authors believe that since the A/C is such a small joint, the human shoulder (under normal circumstances) could actually function adequately without it. However, long-term A/C restrictions can have devastating affects on all upper limb functioning.
Since the acromioclavicular is a planar joint, small movements occur in all three planes. Arm elevation causes the acromion to glide superiorly on the distal clavicle. To test movement of this joint on yourself, simply glide your right index finger laterally along the superior surface of your left clavicle beginning at the sternoclavicular joint. Just before you contact the acromion you should feel a bump or a notch. Since arm elevation raises the acromion in relation to the clavicle, left arm abduction should allow your finger to palpate a “dip” as the acromion rises on the clavicle.

Approximately 20° of motion occurs at the AC joint during arm abduction with 10° occurring between 0° and 30° of arm elevation and the last 10° occurring during the last 45° of the normal range (180°) of arm elevation. At both the AC and SC joints, the clavicle posteriorly rotates approximately 45° during arm elevation. This motion is allowed by the planar configuration at the A/C joint and the fibrocartilaginous articulating disc between the sternum and proximal clavicle as discussed in the last “Sternoclavicular” newsletter.
The most common three restrictions at the acromioclavicular joint involve limited internal and external rotation and abduction. To test for restrictions of internal and external rotation, the client’s elbow is flexed 90 degrees, arm horizontally abducted 90 degrees, and horizontally adducted 30 degrees. Adducting the arm 30 degrees close-packs the glenohumeral joint allowing the therapist to isolate and test only for A/C restrictions.
Assessing for Internal Rotation Restrictions

To test for limitations in internal rotation the therapist’s left-hand braces medial to the A/C joint, shoulder braces elbow, and his right hand brings client’s arm to the first internal rotation barrier. The client attempts external rotation (pushes up) with a 20% effort to a count of six and relaxes. The therapist then brings the arm down into more internal rotation to the next restrictive barrier and repeats the same procedure until full 90 degrees of internal rotation is restored.
Assessing for External Rotation Restrictions
The therapist’s right-hand braces the AC, arm braces the elbow, and his left hand brings client’s arm to the first external rotation barrier. Therapist resists clients attempt to internally rotate (pushing arm down) to a count of six and relaxes. Client’s arm is then brought up to meet the new external rotation barrier and procedure is repeated until 90 degrees of external rotation is achieved. The key to success in this maneuver requires that therapist always maintain the arm in 30 degrees of horizontal adduction so the glenohumeral does not come into play.
Testing Arm Abduction
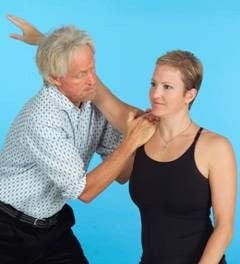
Now it is time to test the ability of the arm to abduct in a smooth 180 degree pain-free arc. In this test, the client’s right arm rests on therapist’s left shoulder and is brought into 30 degrees if horizontal abduction. Therapist bends knees and hands grasp medial to the acromion. As the therapist slowly straightens his legs while bracing with his hands, a counter-force is created that brings the client’s arm to the first abduction restrictive barrier. Client is asked to press down on therapist’s shoulder to a count of six and relax. Therapist again straightens legs bringing client’s arm up to the new restrictive barrier. This continues until 180 degrees of smooth, pain-free abduction is attained.
AC joint restrictions typically limit end-range elevation and cross-body adduction. Often seen in long-standing rotator cuff and frozen shoulder dysfunctions, sternoclavicular and acromioclavicular restrictions are typically the first joints affected by postural asymmetries (upper crossed syndrome) in the upper quadrant. As a result, even minor restrictions at these primary upper extremity joints set off mechanoreceptive muscle/joint reflex arcs that quickly travel down the kinetic chain producing sympathetic protective muscle guarding (splinting) in all soft tissues and associated joints of the shoulder. Pain-spasm-pain cycles are often difficult to correct until full range of motion is restored to these commonly overlooked bony articulations.
Note: In all the ‘so-called’ joint mobilization routines presented during our tour through the upper extremities, please keep in mind that although we are speaking in terms of bony restrictions, our intent is to release myofascial adhesions limiting joint movement.