Introduction
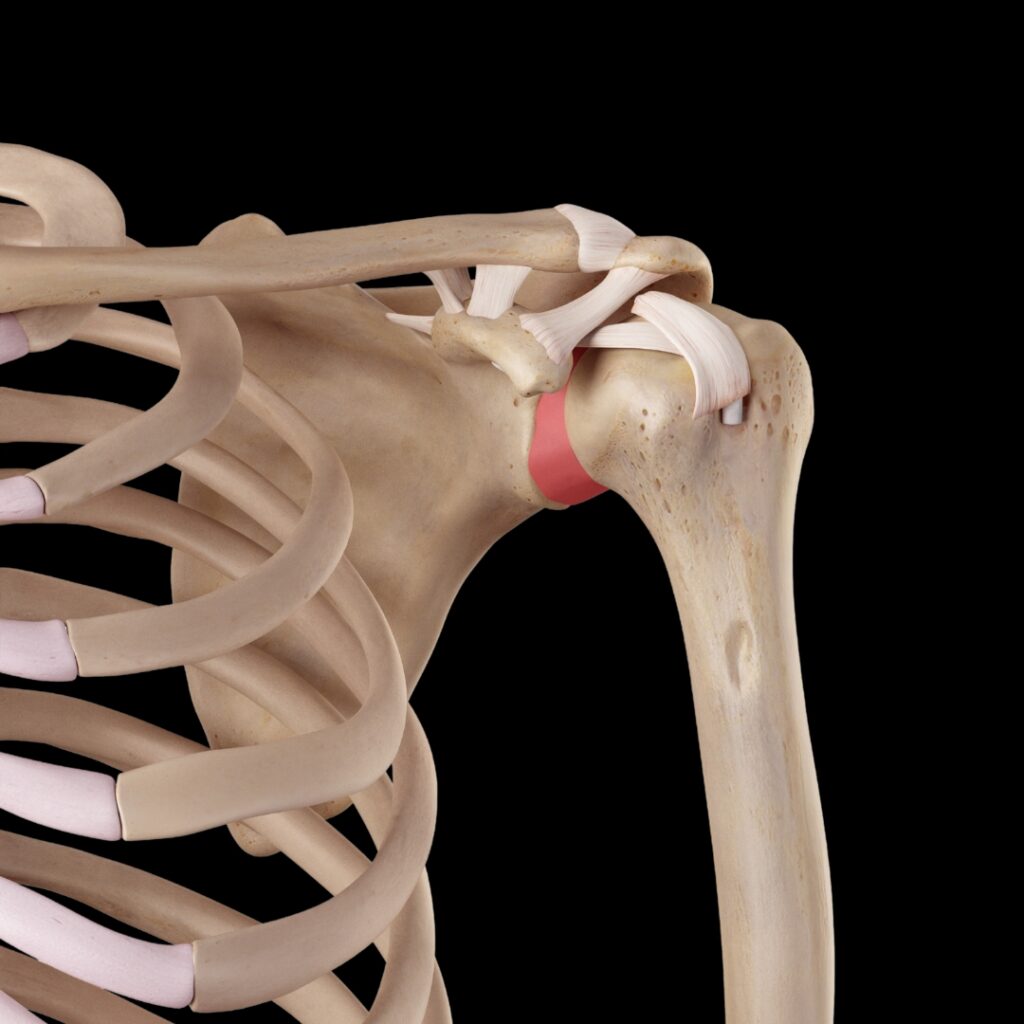
Healthy shoulder motion depends on a finely coordinated relationship between mobility and stability. The shoulder girdle is designed for remarkable range of motion, but that freedom comes with a tradeoff. Unlike the hip, where the femoral head sits deeply in the acetabulum, the humeral head rests against a relatively shallow glenoid fossa. This design allows the arm to move through large arcs of motion, but it also requires precise neuromuscular control to keep the humeral head well-positioned during movement.
Ideal shoulder girdle balance requires some muscles to act as stabilizers and others as mobilizers, depending on joint position, load, speed, and the demands of the task. These roles are not fixed. A muscle that stabilizes during one movement may become a prime mover or decelerator in another. When these coordinated relationships work well, the shoulder maintains optimal alignment through motion. This is often described as joint centration.
Joint Centration
Joint centration means the articular surfaces stay well-aligned as the joint moves. A useful comparison is the wheel on a car. When the center of rotation is aligned with the center of the hub, the wheel spins smoothly and efficiently. When that alignment is altered, the wheel may still turn, but it does so with increased strain, drag, and mechanical wear. In the shoulder, loss of centration may change how the humeral head glides, rolls, and compresses within the glenoid fossa. Over time, this can contribute to irritation, guarding, and inefficient movement patterns.
Altered Alignment and Function
We commonly see this in upper crossed syndrome postures, where a forward head carriage, rounded shoulders, increased thoracic flexion, and altered scapular positioning change the way the shoulder girdle organizes itself. The scapula may sit in a more protracted, anteriorly tilted, or downwardly rotated position. In some clients, this contributes to scapular winging or poor scapulohumeral rhythm. When the scapula does not upwardly rotate, posteriorly tilt, and externally rotate well during arm elevation, the glenoid is not positioned as efficiently to support the moving humeral head.
It is important to be accurate here. Research has not shown a simple one-to-one relationship between posture and rotator cuff impingement or tendinopathy. Many people with rounded shoulders have no pain, and many people with rotator cuff pain do not present with a textbook upper crossed posture. Still, in clinical practice, suboptimal postural habits often appear to play a meaningful role in loss of shoulder function, especially in clients who perform repetitive or overhead activities. Posture may not be the sole cause, but it can influence joint position, muscle recruitment, proprioception, and the available range of motion.
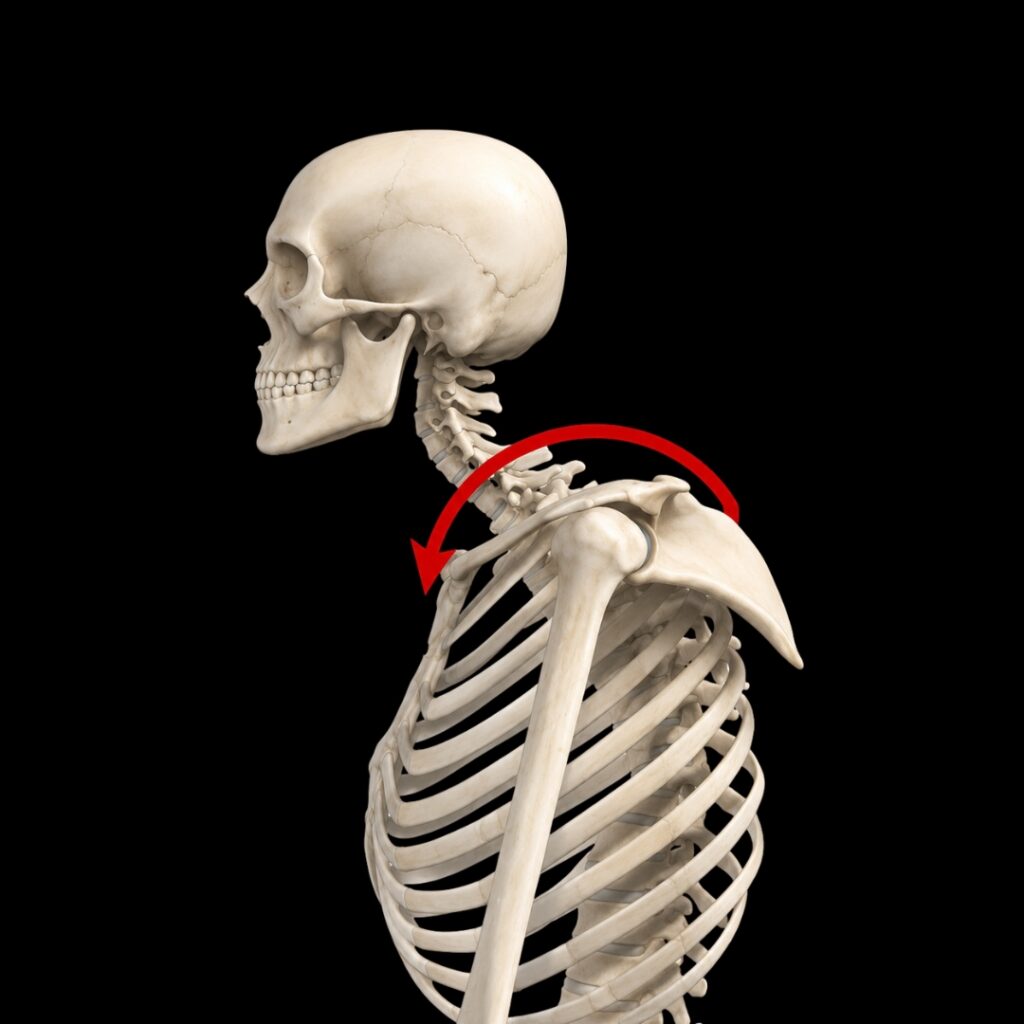
Try this simple experiment. Stand in a tall “military” posture with the shoulders gently back, the sternum lifted, and the chin slightly tucked. Close your eyes and abduct your arms out to the side and overhead as far as comfortably possible. Notice the ease and range of motion. Now slump into a forward head posture with the chin jutting forward, the thoracic spine rounded, and the arms internally rotated. Close your eyes again and raise your arms overhead. Most people notice an immediate decrease in range. Some feel strain around the lateral shoulder or rotator cuff region near 90 degrees of abduction. This is not necessarily pain or pathology. It is a demonstration of how quickly altered alignment can change shoulder girdle function.
The Rotator Cuff and Joint Centration
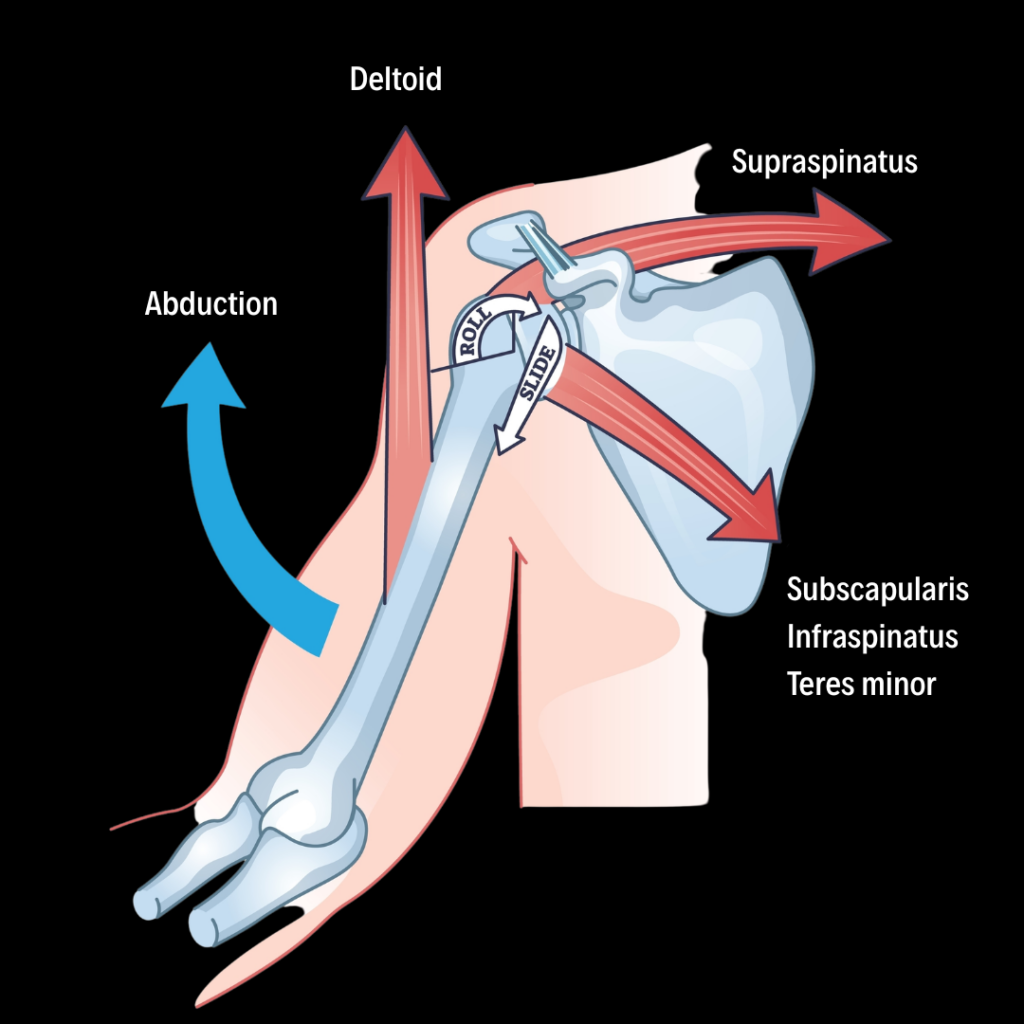
The rotator cuff includes the supraspinatus, infraspinatus, teres minor, and subscapularis. These muscles do much more than rotate the arm. One of their most important jobs is to help maintain the humeral head in a centered relationship with the glenoid fossa during movement. They do this through a mechanism often described as concavity-compression. In simple terms, the cuff compresses the rounded humeral head into the shallow concavity of the glenoid while also guiding its movement.
During arm elevation, the deltoid generates a powerful upward pull on the humerus. This is necessary for abduction and flexion, but if the deltoid acts without adequate rotator cuff control, it may create a superior shear force that translates the humeral head upward. The cuff muscles help counterbalance this tendency. They compress, steer, and stabilize the humeral head so it can roll and glide efficiently rather than migrate excessively toward the acromion.
This is where shoulder girdle balance becomes essential. In rounded shoulder postures, the scapula and glenoid may be positioned in a way that alters the mechanical environment of the shoulder. The nervous system may respond by increasing tone in muscles such as the upper trapezius, levator scapulae, pectoralis minor, and deltoid. These muscles are not “bad” muscles, but when they dominate a movement pattern, they can overpower or interfere with the stabilizing role of the rotator cuff and lower scapular stabilizers.
This imbalance may contribute to what we can call a deltoid shear pattern. In this pattern, the deltoid’s superior pull is not adequately balanced by the rotator cuff and scapular stabilizers. The humeral head may ride high in the glenoid during abduction, increasing compression in the subacromial space. At or near 90 degrees of abduction, this may increase irritation of tissues such as the supraspinatus tendon, subacromial bursa, or long head of the biceps tendon. Over time, repeated compression and poor load distribution may contribute to tendon irritation, protective guarding, fibrosis, or tendinopathy.
From Tissue Tension to Sensorimotor Dysfunction
Poor shoulder mechanics may begin as a tissue issue. A client may develop pectoral tightness from prolonged sitting, rotator cuff irritation from overuse, thoracic stiffness from habitual flexion, or protective guarding after trauma. However, persistent shoulder dysfunction is rarely only about tight tissue. Over time, it becomes a sensorimotor problem.
The nervous system relies on accurate information from joints, muscles, fascia, skin, and connective tissue to organize movement. When joint motion is restricted, muscle tone is altered, or pain is present, proprioceptive input may become less reliable. The brain then has to make movement decisions based on incomplete or distorted information. This can lead to protective guarding, altered recruitment patterns, reduced confidence in movement, and further loss of range.
In this way, shoulder dysfunction can become self-sustaining. A stiff joint changes muscle function. Altered muscle function changes joint loading. Poor joint loading changes proprioceptive feedback. The nervous system responds with more guarding, and the cycle continues.
For this reason, the separate activity of individual muscles is less important than their coordinated activity within functional movement patterns. The goal is not simply to stretch what feels tight or strengthen what appears weak. The goal is to restore the shoulder girdle’s ability to move, stabilize, and adapt.
Mobility First
When working with rotator cuff pain, shoulder stiffness, or upper crossed patterns, it is tempting to move quickly into strengthening exercises. But strengthening a joint that is not moving freely may reinforce faulty mechanics. If the humeral head is not centrating well, if the scapula is not moving efficiently, or if the thoracic spine cannot extend and rotate, strengthening may add load to an already compromised system.
This is why the myoskeletal approach emphasizes mobility first. Before asking a client to strengthen the shoulder, we want to help restore the joint and soft tissue conditions that allow the shoulder to move well. This may include improving thoracic mobility, reducing pectoral and anterior shoulder restriction, decompressing guarded tissues around the neck and shoulder girdle, restoring scapular glide, and improving glenohumeral joint play.
Passive stretching of noncontractile capsular tissue may help in some cases, but it is usually only one part of the solution. Active movement is essential. When clients actively move through newly available range, they reinforce the idea that the arm can move safely. This has both psychological and physiological value. Psychologically, active motion builds confidence and reduces fear of movement. Physiologically, it helps organize collagen along functional lines of stress, improves local circulation, nourishes articular cartilage through synovial fluid movement, and supports restoration of strength and coordination.
Mobilization with movement is especially valuable because it combines manual input with active client participation. The therapist helps guide the joint or soft tissues while the client performs a pain-free or reduced-pain movement. This gives the nervous system novel, corrective input. The client does not simply receive the technique. They participate in relearning the movement.
MAT Techniques
Try these three techniques to improve shoulder girdle balance. These techniques are designed to improve mobility, reduce guarding, and restore more efficient shoulder girdle mechanics. Once proper glenohumeral and scapulothoracic mobility improves, home retraining may include exercises for core stability, scapular stabilization, thoracic extension, and rotator cuff strengthening.

GTO Release of the Lateral Arm Fascia
The client is laying on their left side, while you stand behind them at their hips facing toward the top of the therapy table. Reach back with your left hand to grasp the client’s right wrist. Place your soft forearm above the client’s elbow and sink into the fascia.
Traction the client’s arm with your left hand at the wrist while you slowly strip the fascial bags up toward the medial deltoid and stop when you feel the acromion process.
Friction the tendoperiosteal junction of the supraspinatus tendon by rocking your forearm across the tendon for 20 seconds. Then hold for a Golgi Tendon Organ (GTO) release. Repeat this procedure three to five times.

Webbing Technique to Drop the Humeral Head
The client is laying on their left side, while you stand behind them at the top of the therapy table. Grasp the client’s right elbow with your left hand. Use the web of your right hand to contact the humerus just below the acromion process.
Gently pull the client’s elbow while pushing the humerus with your webbed hand. This creates a counterforce between the two hands. Ask the client to inhale and gently pull their elbow toward their hip to a count of five against your resistance. As the client exhales, maintain the counterforce to encourage the correct positioning of the humeral head in the joint capsule.


Shoulder Decompression
The client is prone with their right arm resting comfortably behind their back. Stand on the client’s right side. Slide your right hand under the client’s anterior shoulder near the anterior deltoid. Place your left hand on the client’s scapula to create a firm counterforce between your two hands.
Ask the client to inhale and gently press their shoulder toward the therapy table using about 20 percent effort. Resist this effort with your right hand while your left hand braces the scapula.
As the client exhales and relaxes, gently pull the anterior shoulder superiorly and posteriorly with your right hand while your left hand guides the scapula into depression and retraction. This counterforce helps stretch the pectoralis major, reposition the scapula, open the anterior chest wall, and decompress the sternoclavicular, acromioclavicular, and glenohumeral joints.
Repeat three to five contract-relax repetitions, then perform the technique on the opposite side.
Special Savings this week only!
Save 25% off the "Myoskeletal Mobilization Massage Course"

If you could learn one routine from Erik Dalton that you’d use every day, this would be it. The Myoskeletal Mobilization Massage course is a “greatest hits” collection of over 80 techniques designed to improve mobility, reduce pain, and keep your own body feeling strong. Follow along step-by-step through a full-body routine you can immediately bring into your practice. Whether you want to enhance relaxation sessions or integrate more clinical results, this course gives you both. Save 25% this week only.
Sale ends Sunday, July 5th. Bonus: Purchase the home study course and receive the eLearning course for FREE!