Leveling the Head and Tail
Since most SI joints only move about 2 to 4 millimeters during weight bearing and forward bending, they are described as a gliding-type joint. This motion is quite different from the hinge-type articulation at the knee or the ball-and-socket motion of the hip. Considered a viscoelastic joint, the SI’s major movement comes from ligamentous stretching. Therefore, its primary function within the pelvic girdle is to provide shock absorption for the spine by stretching in various directions. When sacroiliac joints work in perfect harmony with the third bony articulation of the pelvis (symphysis pubis), a marvelous self-locking mechanism develops that helps us walk. Aided by power generated by the hip abductors (gluteus medius/ minimus, TFL and piriformis), the pelvic joints brace the weight-bearing side during gait. This locking system, termed force closure, allows smooth transference of body mass from one leg to the other. Although no muscles directly bind down the three pelvic joints, when working synchronously with the SI ligaments they provide the pelvis − “the great adapter” − with a remarkable antigravity springing system that can absorb both ascending and descending forces (Fig. 1).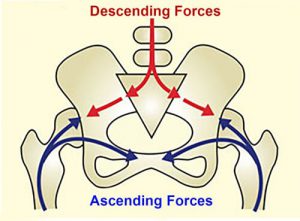
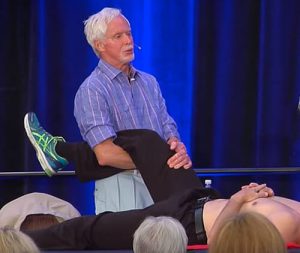
During the aging process, there is an increase in the grooves on the opposing surfaces of the sacrum and ilium, which reduces available motion of the SI joint. This is a perfect example of the body’s innate wisdom attempting to sacrifice complexity of motion for stability. Although the three bones of the pelvis frequently are at the seat of a “primary” lesion, I have found that a missing key in successful correction of recurrent SI pain is motion-restricted hip joints, i.e., poor alignment of the femur in the acetabulum. For the pelvis to effectively absorb the forces imposed upon it, the hips must be aligned and functioning properly (Fig.2).

A stable pelvis, achieved through proper upper and lower quadrant balance, is essential for long-term correction of low back conditions. In the presence of pelvic instability, the brain may try to stabilize the lumbosacral joint by layering the area with protective multifidus muscle spasm, but it does little good to try and release hypertonic spasm in these spinal groove stabilizers until the pelvic alignment problem is corrected. Myoskeletal techniques for hip and back pain include low-force mobilization and graded-exposure stretching to help the brain recognize and reorganize neural input to the affected area.
These techniques are part of this year’s “Leveling the Head and Tail” workshop June 30 – July 2 in Oklahoma City. Special guest James Waslaski treating rotator cuff and frozen shoulder injuries.
Iliosacral Alignment Routine
GOAL: Create joint play in SI Joints
LANDMARK: Pelvic bowl
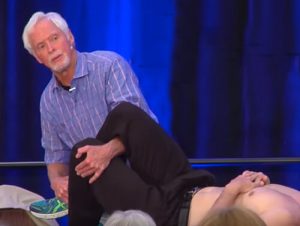
 A. ACTION: (Client Supine)
• Therapist stands on client’s right with arm lock maneuver
A. ACTION: (Client Supine)
• Therapist stands on client’s right with arm lock maneuver
• With client’s right knee flexed and foot resting flat on the table, therapist snakes his right arm over and through his popliteal space.
• Therapist’s left hand braces client’s anterior thigh so the flexed hip can be internally/externally rotated, abducted/adducted, and compacted/distracted.
• Therapist pulls (distracts) client’s thigh to posteriorly rotate the right ilium and compacts to anteriorly rotate .
• Client is asked to pull his hip toward the table to a count of five and relax.
• Therapist leans body weight back to distract/decompress fixated hip capsule.
Note: To avoid contact with breast tissue, therapist can place client’s knee in armpit
 B. ACTION: DonTigny SI-joint Release # 1
B. ACTION: DonTigny SI-joint Release # 1
• With client’s knees flexed and feet resting on the table, therapist’s left arm snakes under client’s right knee and grasps his contralateral thigh just above the knee.
• Therapist’s right hand grasps client’s right ankle and de-rotates ilium by lifting his hip with left arm while pushing down on her ankle.
• Therapist leans both knees away from him so the “line-of-drive” is inferior and medial
• Client is asked to hip-hike his right ilium against therapist’s resistance to a count of five
• Client relaxes and therapist pulls the right knee inferomedially.
• This counterforce posteriorly rotates the client’s right ilium while the medial force helps mobilize a fixated right SI-joint .
These techniques and more can be found in the Lower Body Home-Study
![]()
On sale this week only!
Save 25% off the Upper Body Course!

NEW! Enhanced video USB format!!!
Learn unique approaches to work with the shoulder girdle, arms, neck, and torso, this course will prepare you to relieve painful myoskeletal issues in the upper body. Through video demos and animation, you’ll learn to identify several compensatory movement patterns and their associated reflexogenic pain. With this understanding of where the true source of problems arise, you’ll be able to develop highly effective treatment protocols and deliver lasting results. This course provides you with the skills you need to confidently relieve pain issues in the upper body. (20 CE)
Bonus: When you order the Home Study version, get the eLearning course and and an additional 2CE Ethics eCourse for free!
Save 25% off the Upper Body Course this week only. Offer expires Sunday, March 1st. Click the button below for more information and to purchase the course for CE hours and a certificate of completion to display in your office.







