Mobilizing the ulnar nerve
by Erik Dalton
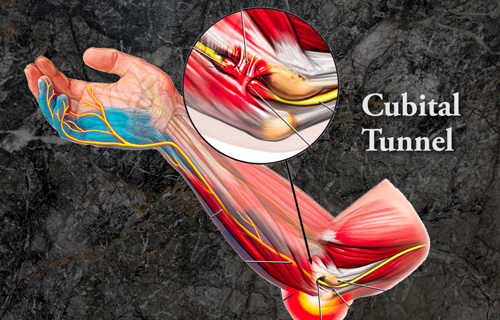
The ulnar is the most exposed of all nerves and ranks second only to the median nerve (carpal tunnel syndrome) as an arm and hand pain generator. Irritation of the ulnar nerve can present as tingling, pain and numbness in the pinky and ring fingers sometimes in a shocking way as the flexed elbow strikes an object compressing it against bone. Like a telephone cable, the ulnar nerve passes through a protective tunnel behind the elbow’s medial epicondyle or funny bone forming what is called the ‘cubital tunnel’. When the ulnar nerve is compressed or entrapped, the nerve can tear and become inflamed leading to a variety of symptoms, called Cubital Tunnel Syndrome. (Figure 1)
I’ve discovered about eight ulnar nerve entrapment sites beginning in the neck, extending through the thoracic outlet, armpit, and down into the hand. All those entrapment sites are addressed in my new “Treating Trapped Nerves” home-study course, and some examples are presented below. You’ll love how easily these routines integrate into your existing massage and bodywork practice, and your clients will be amazed at how quickly they are free of nagging pinched nerve pain emanating from the neck, thoracic outlet, cubital tunnel, Guyton’s tunnel, carpal tunnel, and sciatic nerve.
Ulnar Nerve Mobilization (C7, C8, T1), Cubital tunnel

Soft Tissue Prep
ACTION: (Figure 2)
- To release ulnar entrapment under the subscapularis muscle, therapist’s left hand grasps client’s wrist and abducts arm, while soft flat fingers of therapist’s right hand contact subscapularis muscle in armpit
- As therapist steps to his left, he flexes and internally rotates client’s arm so soft flat finger pads (or fist) can stretch the subscapularis
- As he steps right, the fingers are repositioned so his fingers can work all the attachments that may be entrapping the ulnar nerve
- Next, the therapist’s thumbs strip up and down the flexor carpi ulnaris, while client flexes and abducts the arm and extends the wrist
- Therapist’s thumbs then move up to the olecranon and thumb’s strip fibrotic tissues (including pronator teres) while the client extends, abducts and brings the palm toward side of face (fingers down)
- Therapist grasps the cubital tunnel muscles while his opposite hand slings and resists (S & R)
- Repeat this maneuver 5 times and reassess for improved tissue mobility

Ulnar Nerve Gliding Routine
ACTION: (Figure 3)
- With therapist facing his client, his right hand grasps client’s right wrist, and horizontally abducts and externally rotates her arm to 90 degrees
- Therapist’s left hand snakes under and grasps/depresses the client’s shoulder to stabilize
- Client’s elbow is braced against therapist’s hip
- The fingers of therapist’s right hand radially deviate and extend client’s wrist and fingers (particularly the 5th digit)
- In this position, the client right rotates / sidebends her head to gently stretch the nerve
- Therapist then uses his hip and hands to slowly abduct and depress client’s shoulder a little further testing for increased nerve sensitivity
- To glide the ulnar nerve proximally, the client left sidebends her head as the therapist releases finger and wrist extension
- To glide nerve distally, the therapist increases elbow flexion, and arm and wrist pronation (goal is to place client’s fingers along the side of her face with fingers facing down)
- Slowly repeat 5 to 10 times to gently floss and release entrapped nerve at the thoracic outlet, cubital tunnel, or Guyon’s canal.
- Repeat this maneuver 5 times and reassess, for decreased ulnar nerve pain
On sale this week only!
Save 25% off the Upper Body Course!

NEW! Enhanced video USB format!!!
Learn unique approaches to work with the shoulder girdle, arms, neck, and torso, this course will prepare you to relieve painful myoskeletal issues in the upper body. Through video demos and animation, you’ll learn to identify several compensatory movement patterns and their associated reflexogenic pain. With this understanding of where the true source of problems arise, you’ll be able to develop highly effective treatment protocols and deliver lasting results. This course provides you with the skills you need to confidently relieve pain issues in the upper body. (20 CE)
Bonus: When you order the Home Study version, get the eLearning course and and an additional 2CE Ethics eCourse for free!
Save 25% off the Upper Body Course this week only. Offer expires Sunday, March 1st. Click the button below for more information and to purchase the course for CE hours and a certificate of completion to display in your office.







