Increased outdoor activity during the summer months tends to escalate the number of overuse and traumatic injuries seen in massage and bodywork practices. One of the most common of these is sacroiliac joint syndrome (SIJD). The SI joint is susceptible to traumatic (sudden, forceful injury) and inflammatory conditions. Common causes of injury are slips or falls; however, it also can be injured by overuse. Overuse can result from frequent and prolonged bending or sitting for extended periods of time. Occasionally, intense hip pain and spasm can arise from doing something as simple as bending over to pick up a pencil or tie a shoe.
Injuries of this type can produce ligamentous laxity and allow painful abnormal motion. SI joint hypermobility pain can also be caused by leg length discrepancy, gait abnormalities, prolonged vigorous exercise, and trauma. In any case, the resulting dysfunction disrupts the kinetic chain in which the sacroiliac joint is a key link.
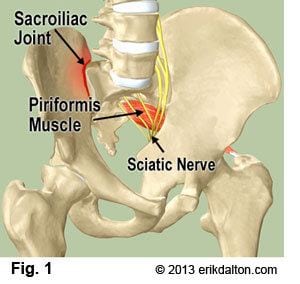
Even though the most powerful muscles in the body surround the SIJ, these muscles influence SI motion only indirectly (Fig. 1). However, the effect the SIJ has on these muscles can be profound. The piriformis, iliopsoas, gluteals, quadratus lumborum, and hamstrings can all be affected to various degrees. With SIJD, these muscles can become tense or spastic, ceasing to perform effectively. This further compromises gait and can lead to development of spinal dysfunction, hip bursitis and leg pain.
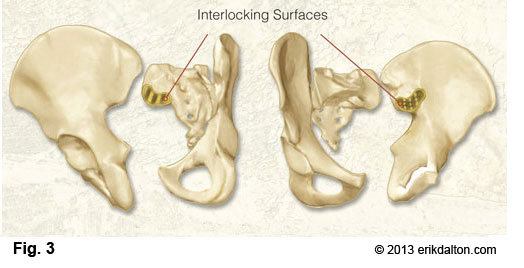
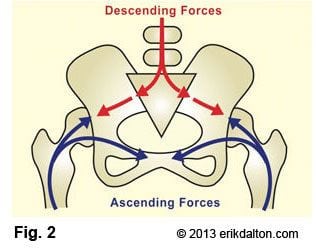
Being a transitional structure (Fig. 2), the SIJ can be thought of as either the bottom of the spine or the top of the leg; it really functions as both. The joint is not very large, especially considering the forces which cross it. What accounts for its stability are its irregular joint surfaces, wedge-like shape of the sacrum, and most importantly, the binding ligaments – the SIJ ligament complex (Fig. 3). These ligaments, considered the strongest ligaments in the body, function like the cables of a suspension bridge. In order for the joint to function properly, each “cable” needs to provide a certain degree of tension and support; each plays a role in bridging the spine to the lower extremities, thus providing the stability necessary for fluid gait and normal body function.
In order to successfully treat SIJD, several factors need to be taken into consideration and properly addressed. These include altered joint mechanics, muscle dysfunction, and ligament incompetence. Manual therapy serves to re-educate the body. Various deep tissue and joint mobilizations, some of which utilize the principle of indirect muscle effect on SIJ motion (muscle energy) help to realign the pelvis and spine.
When possible, self-mobilization techniques are taught, enabling the client to restore alignment on their own or with the help of a partner. Instruction in body mechanics and activity avoidance helps prevent recurrent painful episodes.
But, it is important for the massage therapist to restore proper muscle length, tone, strength and coordination. To fully retrain coordination, the brain must relearn aberrant movement patterns and this is not always an easy fix given our flexion-addicted society. Through the Law of Facilitation, the myelin sheath that covers the neurons, over time has re-wired those faulty movement patterns as normal. So, following each deep tissue, myofascial release, and joint stretching session, the client is instructed in specific exercises, including a regimented stretch-strengthen program. This is an essential piece of the puzzle folks.
Tight or spastic muscles inhibit progress and are many times responsible for perpetuating the dysfunction. Aquatherapy is also a useful means of initiating motion recovery and restoring normal movement patterns, particularly when excessive deconditioning or pain is an issue. Although restoring normal function can be extremely challenging, it is never impossible. Myoskeletal Alignment and other similar therapies seek to restore length-strength balance to muscles and enveloping fascia before compensations lead to gait alterations and subsequent low back, hip and leg pain.
For further reading and video, please visit: Sacroiliac Jjoint Syndrome
References
- Postacchini F, Massobrio M, Idiopathic coccygodynia. Analysis of fifty-one operative cases and a radiographic study of the normal
coccyx. The Journal of Bone and Joint Surgery. 1983 65(8): 1116-1124. - Kim NH; Suk KS: Clinical and radiological differences between traumatic and idiopathic coccygodynia.
Yonsei Med J, 1999 Jun, 40:3, 215-20.
On sale this week only!
Save 25% off the Upper Body Course!

NEW! Enhanced video USB format!!!
Learn unique approaches to work with the shoulder girdle, arms, neck, and torso, this course will prepare you to relieve painful myoskeletal issues in the upper body. Through video demos and animation, you’ll learn to identify several compensatory movement patterns and their associated reflexogenic pain. With this understanding of where the true source of problems arise, you’ll be able to develop highly effective treatment protocols and deliver lasting results. This course provides you with the skills you need to confidently relieve pain issues in the upper body. (20 CE)
Bonus: When you order the Home Study version, get the eLearning course and and an additional 2CE Ethics eCourse for free!
Save 25% off the Upper Body Course this week only. Offer expires Sunday, March 1st. Click the button below for more information and to purchase the course for CE hours and a certificate of completion to display in your office.







