Introduction
Human movement is an intricate synthesis of mechanics and neurology, where every functional structure plays a critical role. From the push of a toe to the swing of a hip to the turn of the head, every action comprises small movement events that form a larger sequence in a kinetic chain. In this article, we examine the complexities of the kinetic chain and what happens when a “snag” disrupts the ripple of physiology that propels us through space. We’ll narrow our focus to the role of the foot and the big toe as a pivotal player in kinetic chain dynamics.

What is a Kinetic Chain?
In the most basic terms, movement begins with a signal from the central nervous system (CNS), which activates specific muscle fibers, initiating muscle contractions. Muscles shorten transmitting force to associated bones through their tendons. Bones act as levers (rigid bars that pivot around a point), and joints function as fulcrums (pivot points around which levers move) to facilitate motion. Synergist, antagonist, and stabilizing muscles contract or relax to help control motion or reinforce joints. Throughout this process, proprioceptors in muscles, tendons, and joints send feedback to the CNS about the body’s position, tension levels, and movement speed so the CNS can make rapid, real-time adjustments to refine and coordinate motion.
Movement is seldom isolated to one joint. Instead, movement occurs as a series of actions called a kinetic chain. We can think of kinetic chains as the interconnected system of bones, joints, muscles, ligaments, and tendons coordinated by the nervous system to produce complex movements.
For example, when we initiate a step, the iliopsoas and rectus femoris contract to flex the hip while the hamstrings contract to flex the knee, reducing the limb’s length so the foot can clear the ground.
As the brain prepares for the foot to contact the ground, the gluteus maximus and quadriceps contract to straighten the knee while the tibialis anterior fires to dorsiflex the ankle ensuring the heel hits the ground first. The quadriceps continue to contract to control knee flexion while the soleus and gastrocnemius contract to stabilize the ankle.
The ankle moves into plantar flexion after the heel strike, while the knee flexes slightly. As the body’s weight moves over the foot, the calf muscles contract forcefully to plantarflex the ankle and lift the heel off the ground as the toe flexors engage to propel the body forward.
As one leg goes through the swing phase, the opposite leg goes through the stance phase. At the same time, the gluteus medius and minimus keep the pelvis level, while the torso and arm muscles work to maintain balance and assist forward propulsion. Each small event must happen in the proper sequence and to the proper degree for coordinated movement.

What Happens When There’s a Kink in the Chain?
As we contemplate the small movement events that lead to walking or running, it’s easy to imagine how one minor dysfunction creates imbalances that might have profound results. What if a hip joint is restricted? What if the gluteal muscles are weak? What if a ligament is lax? Now, all structures in the kinetic chain must compensate as best they can. Some structures along the chain may be unable to dissipate or absorb forces properly, exposing them to repetitive stresses they weren’t designed to withstand. Snags in the kinetic chain cause a knee problem to lead to a hip problem, a hip problem to cause low back issues, and so forth.
Poor Foot Mechanics and the Kinetic Chain
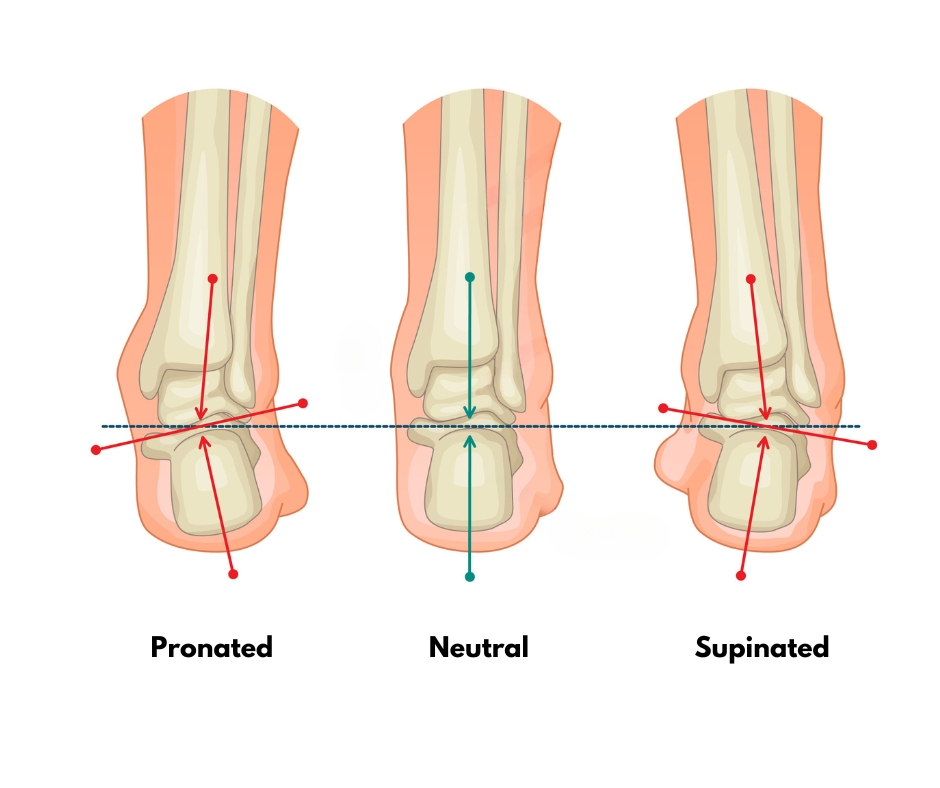
Poor foot mechanics can have a substantial impact on the entire body. The feet are the foundation of the body, and a problem at the base can lead to a cascade of compensatory changes up the kinetic chain. For example, pes planus (flat feet) causes overpronation and leads to internal rotation of structures of the lower extremities, affecting the knees, hips, and back. Pes cavus (high arches) can lead to supination, contributing to issues like plantar fasciitis and shin splints.
The metatarsophalangeal (MTP) joints are critical components in the kinetic chain of the lower limb and play a pivotal role in the “windlass mechanism.” The windlass mechanism is a biomechanical concept explaining how the foot adapts during locomotion to provide flexibility and rigidity at different phases of the gait cycle.
During gait, as the heel touches the ground and the foot starts to bear weight, the plantar fascia is relatively relaxed, allowing the foot to adapt to surfaces and absorb shock. As the body moves over the foot, the toes begin to extend, pulling on the plantar fascia and causing it to tighten and shorten. As the plantar fascia tightens, it elevates the medial longitudinal arch of the foot, transforming the foot into a more rigid structure. The increased rigidity aids in efficient energy transfer and propulsion during the toe-off phase of gait by turning the foot into a lever, facilitating a powerful push-off.
Adequate mobility in the toes, particularly the big toe, is crucial for proper foot mechanics. The first MTP joint should be able to extend as much as 65 degrees, but many people lack full range of motion, causing plantar fascia issues and contributing to “mystery” foot, ankle, knee, and hip pain.
Hallux Limitus and Hallux Rigidus
Hallux limitus and hallux rigidus are related degenerative joint conditions that affect the metatarsophalangeal joint of the big toe. Hallux limitus is the earlier stage of osteoarthritis characterized by reduced range of motion in the MTP joint, particularly during extension. Common signs and symptoms include mild pain, especially on top of the toe joint, stiffness, the development of a callus under the big toe, and difficulty flexing or extending the toes.
Hallux limitus begins in young adulthood. X-ray evidence shows joint changes in 10% of people between 20 and 34 years of age.1 People over 50 have a higher prevalence, with the condition affecting an estimated 1 in 40 adults.2 Without treatment, hallux limitus worsens over time, and discomfort increases. Protective spasming in calf muscles might further disrupt the kinetic chain and cause pain and dysfunction.
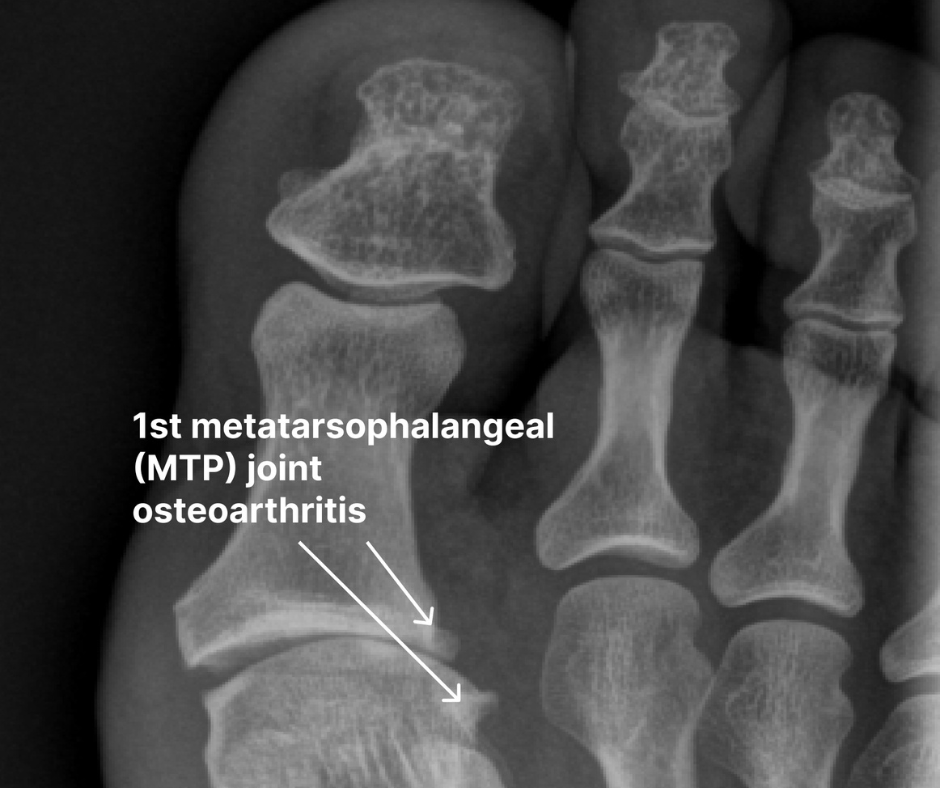
Hallux rigidus is the advanced stage of joint degeneration, where the joint becomes rigid and immovable. This osteoarthritis of the big toe causes joint space narrowing, cartilage loss, bone spurring, and persistent pain, even at rest. Researchers estimate that hallux rigidus affects about 26.7% of people over 50.3
A variety of risk factors predispose people to osteoarthritis in the big toe. Certain foot structures like an elongated first metatarsal bone or flat feet, age (over 50), and gender (women) are primary considerations. Inflammatory joint diseases like rheumatoid arthritis or gout and repetitive stress from sports that include running and jumping are also factors. Finally, previous injury, wearing high heels, shoes with a narrow toe box, or obesity can overload the MTP joints, leading to hallux limitus.
Mobilize the Big Toe as Part of Your Foot Massage
Early intervention can slow or prevent the progression of hallux limitus and improve foot mechanics to support kinetic chain function. Integrating MTP joint movement techniques into your everyday foot massage provides beneficial results.
If the client reports mild pain and stiffness in their big toe, I begin by performing graded exposure stretches to the lower leg muscles to decrease protective muscle guarding. I continue with techniques that warm and mobilize the foot’s soft tissues. Finally, I perform these five MAT movement techniques on both feet to address big toe function directly.

Flexion-Extension
Stand on the left side of your supine client, facing toward the client’s feet. Brace the metatarsal bones with your right hand. With your left hand, grasp the first metatarsal bone at its base and bring the toe into flexion. Then, pull gently on the toe to distract it and bring it into extension. Flex, distract, and extend the toe several times, noticing if there are any grinding sounds or if the movement elicits pain. Always work within the client’s comfort zone and back off if the technique is painful.

Sidebending
Bracing the first metatarsal head with your right hand, use the thumb and fingers of your left hand to slightly sidebend the toe medially and laterally several times within the client’s pain tolerance.

Side-to-Side Translation
Continue bracing the first metatarsal and glide the base of the proximal phalanx to the left without bending the toe and then to the right. Repeat this back-and-forth gliding motion several times within the client’s pain tolerance.

Up-and-Down Translation
While bracing the first metatarsal, glide the base of the proximal phalanx up and down several times within the client’s pain tolerance.

Extension-Rotation
Continue bracing the first metatarsal and slowly distract, extend, and rotate the client’s proximal phalanx bone. Keeping the proximal phalanx bone extended and distracted, medially and laterally rotate the proximal phalanx several times within the client’s pain tolerance.
In Closing
In closing, we’ve examined how mobility limitations in the big toe reverberate up the kinetic chain, causing a domino effect of compensations that lead to stress and pain. By simply including techniques that gently mobilize the big toe in our foot massage routines, we can improve foot mechanics and gait.
References
- Durrant, B., Chockalingam, N. Functional Hallux Limitus. Journal of the American Podiatric Medical Association, 2009.
- Dini M., Parks, CB. Hallux Limitus. In Papadakis, MA, et al eds. Current Medical Diagnosis & Treatment, McGraw Hill, 2024.
- Senga, Y, et al. Prevalence of and risk factors for hallux rigidus: a cross-sectional study in Japan. BMC Musculoskeletal Disorders, Volume 22, Article 786, 2021.