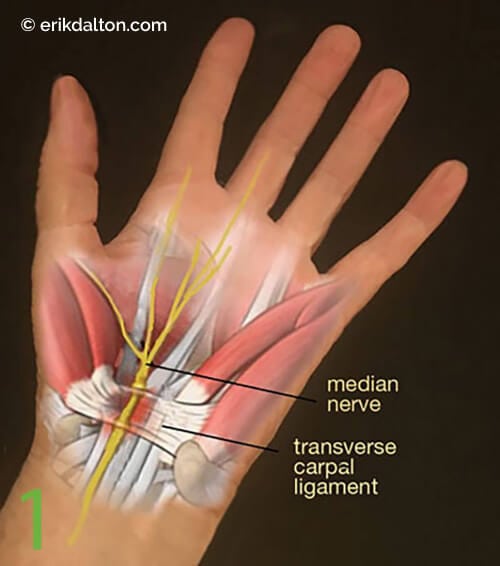
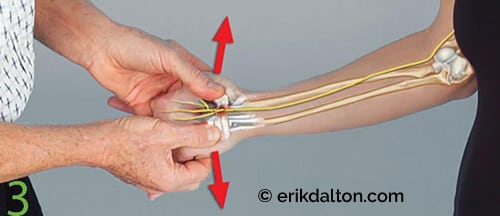
When swollen tendon sheaths and fixated carpals crowd out the median nerve, loss of axoplasmic nutrient flow can trigger chronic inflammation, as well as pain, if the brain feels the injury is a functional threat. A variety of active and passive neural glide techniques exist to help clients with CTS pain, but the flossing routine shown in Image 5. is my favorite. When performing this neurodynamic maneuver, the order of joint positioning is crucial. Begin by stabilizing the shoulder (scapula), followed by the forearm, wrist, fingers, and elbow.