Coccyx pain has been recognized for centuries, with the first documentation appearing in 1588. In 1859, the physician James Simpson coined the term coccydynia to describe pain arising from the coccyx. Today, we know that pain here often follows trauma, such as a fall, a blow during contact sports, or repetitive compression in activities like cycling, rowing, or prolonged computer work. These injuries can cause fractures, dislocations, or abnormal movement at the sacrococcygeal joint, setting off inflammation and degeneration of cartilage. Childbirth is another common cause, as the coccyx becomes more mobile during the final trimester to allow for pelvic expansion. This mobility, while necessary, can also stress muscles and ligaments, producing inflammation and sometimes leading to arthritis in the joint.
Unfortunately, clients who complain of tailbone pain often feel dismissed. Physicians sometimes minimize or belittle these symptoms, with coccyx pain even being referred to as the “lowest form of low back pain.” Yet those who experience it know that it is far from trivial. Coccydynia can make sitting, standing, and even simple daily tasks extremely painful and can reduce quality of life in profound ways.
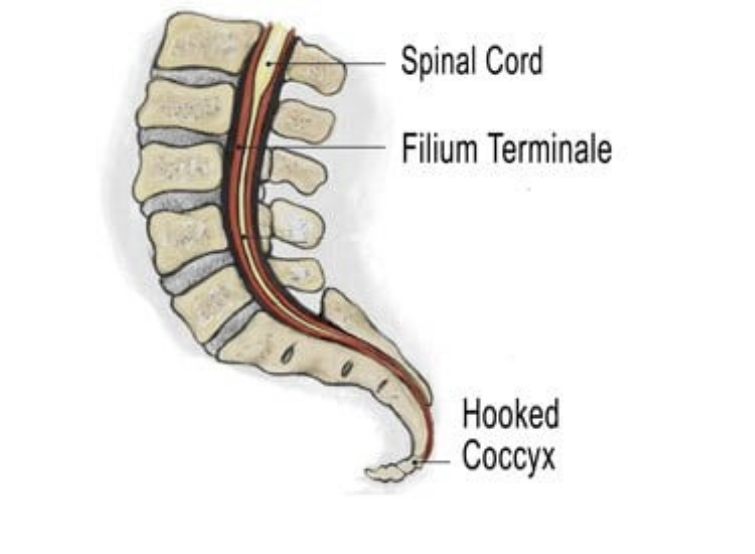
The coccyx is formed from three to five fused vertebrae at the very base of the spine. Functionally, it serves as a shock absorber when sitting, flexing slightly forward as weight is applied to complete the tripod of support formed by the coccyx and the two ischial tuberosities. When misalignment or injury interferes with this function, clients often adapt by leaning forward or to one side in order to shift weight away from the coccyx. This compensation may protect the tailbone, but it can increase stress elsewhere, leading to issues such as ischial bursitis, pelvic imbalance, or chronic lumbar strain.
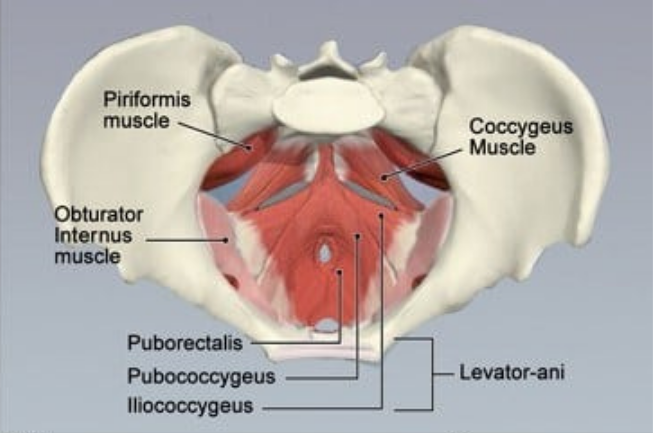
Several important muscles insert at or near the coccyx. On the anterior surface, the levator ani group — including the coccygeus, iliococcygeus, and pubococcygeus — attaches to provide pelvic floor support, maintain continence, and coordinate with the diaphragm for proper breathing (Figure 2). On the posterior surface, the coccyx anchors fibers of the gluteus maximus and connections from the biceps femoris through the sacrotuberous ligament. These muscular relationships make it clear that coccyx dysfunction can influence both pelvic stability and breathing patterns.