Structurally-oriented therapists are keenly aware of the crucial role proper iliosacral alignment plays in preventing compensatory low back and SI joint pain. During the 10-step screening evaluation, therapists usually compare anatomical landmarks such as anterior and posterior superior iliac spines and iliac crests. A commonly observed pattern reveals an anterior/inferior right rotated ilium accompanied by a high left posteriorly rotated ilium. Scientists such as Zink, Previc, Geschwind, Rogers, Vallortigara and Tommasi have developed fascinating theories (motor dominance, cerebral lateralization and genetic potential) to shed LIGHT on the possible origins of these frequently seen patterns. Although most manual therapy clinicians agree that the foot’s architecture plays a major role in iliosacral rotation, aside from lengthening or shortening of a limb, many remain unsure of the link between foot posture, pelvic obliquity and hip/back pain.
A Sham Case Study
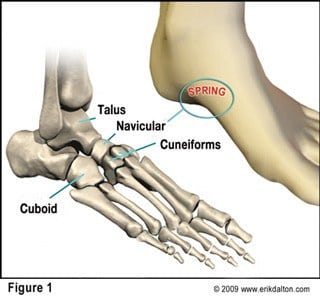
For demo purposes, let’s ‘mock-up’ a postural foot assessment with the client standing. Using the finger pads of your right hand, palpate the medial arch of the left foot. Contact the navicular bone and, with two fingers, attempt to lift the arch checking for joint play (Fig. 1).
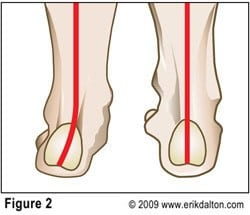
If the navicular and cuneiforms resist this spring test and the mid-foot appears flat, the arch is pronated. As we recall, the most common lower extremity asymmetry is foot pronation. Weakness of tibialis anterior, peroneus longus and the plantar aponeurosis (Stirrup Spring System), results in a valgus subtalar joint (STJ) accompanied by a dropped navicular bone (Fig. 2).
When palpating the navicular on the opposite foot, one discovers a high rigid arch that feels stuck in a supinated position. By viewing the Achilles tendon and calcaneus bone from behind, one observes the subtalar ‘saddle-joint’ cocked in a varus position with body weight shifting laterally and compressing the cuboid. This is the precursor for such conditions as plantar fasciitis and fibular stress fractures. Ideally, at HEEL strike, the foot and ankle ligaments ‘give’ to the pressure allowing the arch to flatten and the tibia to internally rotate. During toe-off, the arch springs open and the tibia externally rotates. Stored potential energy is released in a powerful pulse driving kinetic energy back up through the system to help counter-rotate the torso and pelvis to propel the legs forward.
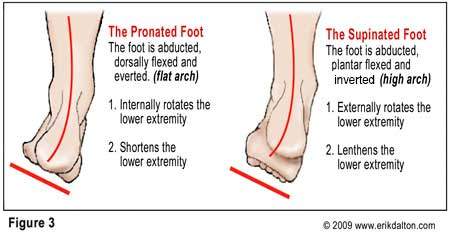
Recall that the term “kinetic CHAIN” describes how we move our bodies. We move in either in an open kinetic chain or closed kinetic chain. The difference lies in whether the moving part is loose in space or fixed against a hard, unrelenting surface…such as the earth. Pronated and supinated feet are an unstable platform and soon encounter resistance further up the kinetic chain. Loss of antigravity spring leads to compensations that torsion and compact the knees, hips, low back, and trunk (Fig. 3).
Femoral Positioning and Pelvic Rotation
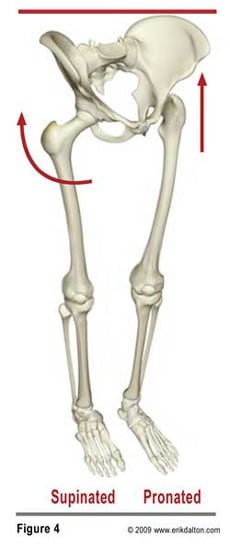
In my experience, the most overlooked and least appreciated area of compensation arises as the femoral heads become asymmetrically positioned in the acetabula. For example, when the pronated left foot internally rotates the thigh and the supinated right foot externally rotates the thigh, one would be walking sideways with each step (Fig. 4). Of course, the body’s sensitive proprioceptors immediately begin left rotating the trunk with the axis of rotation primarily focused at the hips. As the femoral heads reposition in the acetabula, a great amount of stress is placed on the joint capsules, articular cartilages, and supporting ligaments.
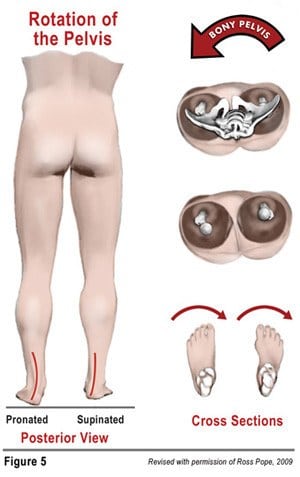
Use a plastic skeleton and pronate the left foot noticing how it internally rotates the left lower extremity causing the femoral neck to follow. This closed CHAIN movement crams the femoral head posteriorly against the back of the acetabulum (Fig 5). Conversely, supination of the right foot externally (right) rotates the femoral neck allowing the head to migrate into the anterior part of the acetabulum. With the right femoral head pushing anteriorly and the left pushing posteriorly, the bony pelvis is forced to left rotate. In this scenario, the high (left) femoral head becomes the axis of rotation as it “drives” the anterior portion of the pelvis upward and backward causing the pelvis to rotate to that side. Thus, the right ilium reacts by dropping on the low femoral head side resulting in an unleveling of the sacral base and a buckling of the lumbar segments.
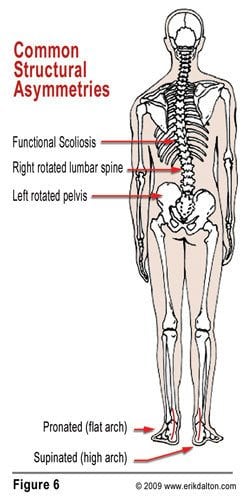
During a screening evaluation, therapists often stop their assessment and begin treating the right anteriorly/inferiorly rotated ilium via hip flexor work followed by QL lengthening techniques designed to drop the elevated left ilium. The ‘fix it as you find it’ approach defies sound structural integrative methodology and is doomed if the torsioned pelvis has roots in foot dysfunction. Notice in Fig. 6 how combined pronation and supination not only torsion the pelvic bowl, but initiate a functional lumbar scoliosis that spreads its tentacles through the thoracic and cervical spines.
Experiment by doing the following: place fingers under each ASIS, pronate your left foot, supinate the right, and feel the right ASIS drop anterior/inferiorly as body weight side-shifts over the left posterior/superiorly rotated innominate. In the absence of hip or lumbar pathology, you should feel the pelvic bowl left rotate.
This mechanism of anteroposterior femoral head positioning also helps explain other clinical findings. For example, we often have clients presenting with bilateral foot pronation (pes planus) complain of back pain. Bilateral pronation increases lumbar lordosis and lumbosacral angle causing excessive compressive force through the L4-5 and L5-S1 facets and intervertebral discs. With these individuals, both femoral heads are positioned posteriorly allowing the pelvic contents to ‘dump’ forward and sway the back. Conversely, bilateral supinated feet position the femoral heads anteriorly in the acetabula resulting in decreased lumbar lordosis, flat back, flat butt and loss of kinetic energy into the ground during gait. Although various aberrant combinations of femoral positioning exist, some are considerably more detrimental than others.
Femoral Positioning and Hip Impingement
At the 15th Combined Open Meeting of the Hip Society and American Association of Hip and Knee Surgeons, held Feb. 28, 2008 in Las Vegas, the ‘godfather’ of femoral acetabular impingement (FAI) Reinhold Ganz, MD, of Bern, Switzerland stated, “Surgical management of hip impingement syndromes is one of the most exciting developments in the entire field of hip pathology and hip disease in the last decade. The key to recognition of FAI is that even minor abnormalities in positioning of the proximal end of the femur can lead to difficult motion and possibly to impingement within the well-constrained hip joint,” During the physical examination, Ganz recommended checking the hip’s internal rotation in flexion using the anterior impingement test. If limited or highly painful when range of motion is executed, this could indicate femoral acetabular hip impingement. 8
Orthopedists theorize FAI could serve as a major cause of damaged hip joints in adults and the primary reason behind the escalation of hip replacements. Treating FAI impingement should involve techniques for balancing femoral head/neck positioning relative to the acetabulum. Since FAI arises from bony or mechanical abnormalities of femoral head placement in the acetabulum, manual therapists often have the best shot in preventing or correcting this anomaly and would benefit greatly by attending workshops designed to assess and treat this pervasive condition.
Summary
A prerequisite need for all pain management, sports, and structural integration therapists should involve a basic understanding of the relationship of iliosacral unleveling and foot posture. Since most therapists are not privy to radiographic measurements, we must develop keen palpatory and visual skills to properly evaluate bony and soft tissue landmarks. As Sir William Osler eloquently stated, “In order to treat something, we must first be able to recognize it”. Any attempt to tackle iliosacral rotational patterns armed with inadequate assessment and treatment TOOLS will undoubtedly end in failure and frustration. From a functional standpoint, there is strong evidence of an associated increase in the incidence of low back pain and hip joint osteoarthritis if foot posture and femoral rotational patterns are not addressed in a timely manner.
In my next “Toolbox of Touch” column, I’ll present theories on “why” we encounter common compensatory patterns; discuss cerebral lateralization and motor dominance, and share Myoskeletal Techniques to address the strain patterns falling within the FAI realm.
On sale this week only!
Save 25% off the Upper Body Course!

NEW! Enhanced video USB format!!!
Learn unique approaches to work with the shoulder girdle, arms, neck, and torso, this course will prepare you to relieve painful myoskeletal issues in the upper body. Through video demos and animation, you’ll learn to identify several compensatory movement patterns and their associated reflexogenic pain. With this understanding of where the true source of problems arise, you’ll be able to develop highly effective treatment protocols and deliver lasting results. This course provides you with the skills you need to confidently relieve pain issues in the upper body. (20 CE)
Bonus: When you order the Home Study version, get the eLearning course and and an additional 2CE Ethics eCourse for free!
Save 25% off the Upper Body Course this week only. Offer expires Sunday, March 1st. Click the button below for more information and to purchase the course for CE hours and a certificate of completion to display in your office.







