Home retraining exercises that focus on restoration of proper tone in the trunk stabilizers, diaphragms, and pelvic floor muscles are essential therapeutic pieces of the pregnancy puzzle. Transversus abdominis, pelvic-clock and Thera-Band toning routines boost therapeutic outcomes when performed on a regular basis between sessions. Pilates, yoga, Rolf Movement and other trunk stabilizing programs also seem effective in helping the body’s innate self-regulatory mechanisms produce a healthy happy baby.
Best Possible Scenario:
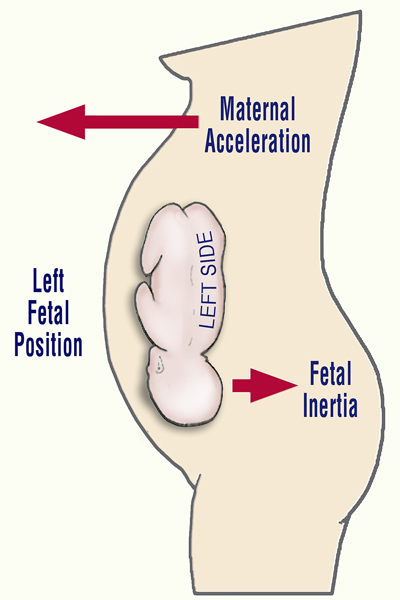
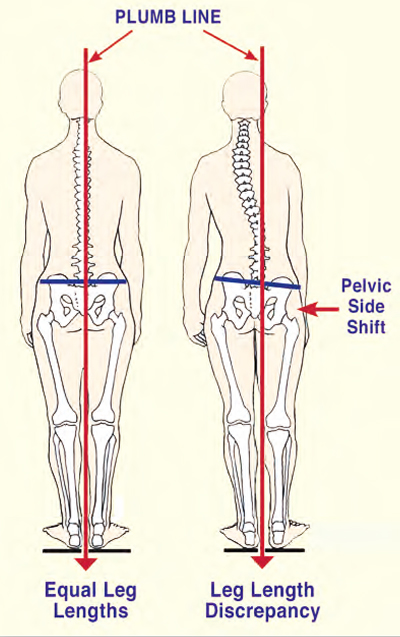
The mother’s best chance for a normal left fetal lie delivery requires that:
- No pelvic bowl asymmetries exist, i.e., sacroiliac, iliosacral, or side-shifted dysfunctions;
- Proper tone be present in the deep trunk stabilizers and lumbar multifidus;
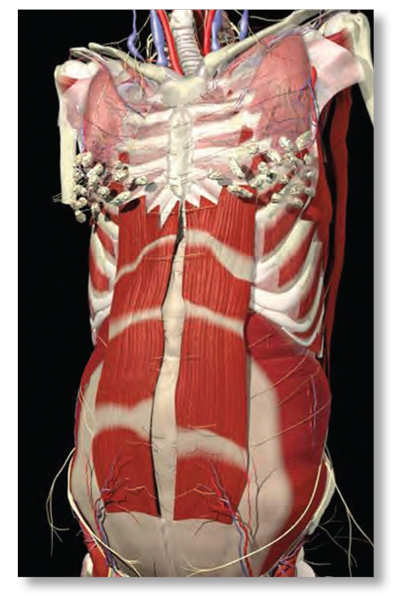
- No spreading (past three fingers’ width) of the recti muscles at midline;
- Obstetrician or midwife directed therapeutic exercises be practiced regularly for adequate abdominal and trunk stabilization support.
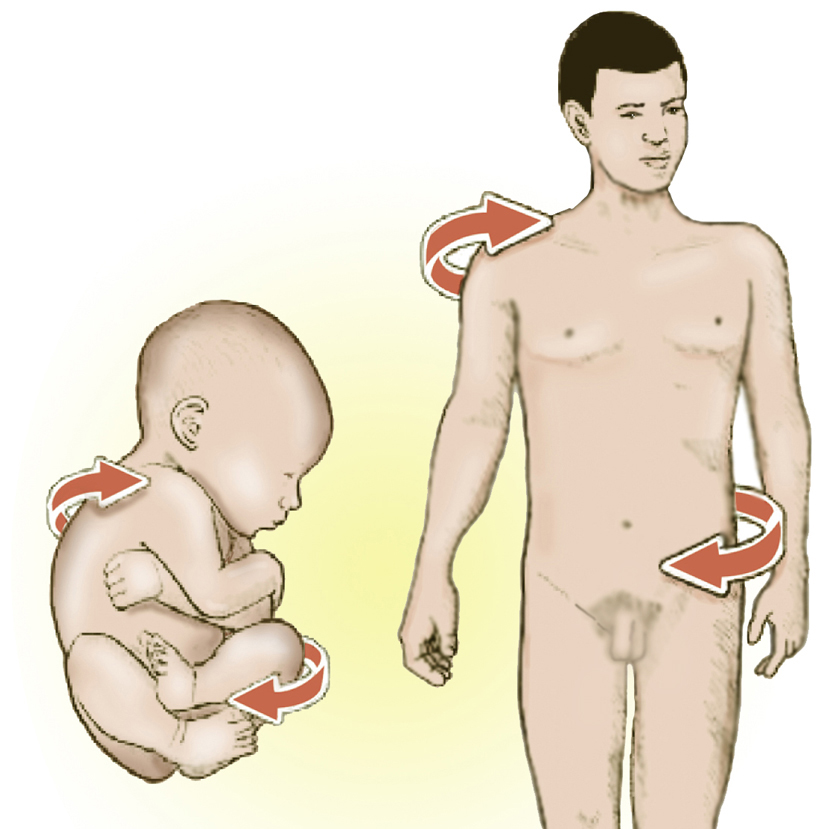
These and other factors will not only help determine the habitus, presentation and delivery of the child, but will also play a major role in proper development and shape of the adult vertebral column. As stated above, early embryologic positioning often forms aberrant fascial rotational preferences that can become exaggerated during one’s lifetime due to life’s little micro and macro traumas. This compensatory process manifests as a loss of range of motion, tissue texture abnormalities (fascial contractures, fibrosis, etc.), and posturally initiated pain. During the final trimester, fascial restrictions can encumber proper blood and lymph flow and create neurological interferences that travel throughout all the body’s soft tissues. Fascial distortions frequently generate pressure gradient alterations in the thoracic outlet, respiratory, and pelvic diaphragms and are major contributors to stagnation in the vascular, lymphatic, endocrine, and respiratory systems. Myoskeletal Zone Therapy incorporates special techniques for eliminating stagnation by restoring optimal diaphragmatic function.
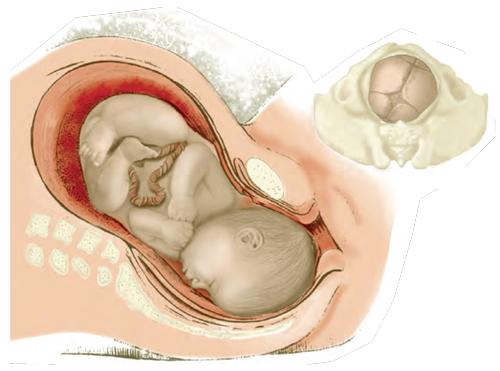
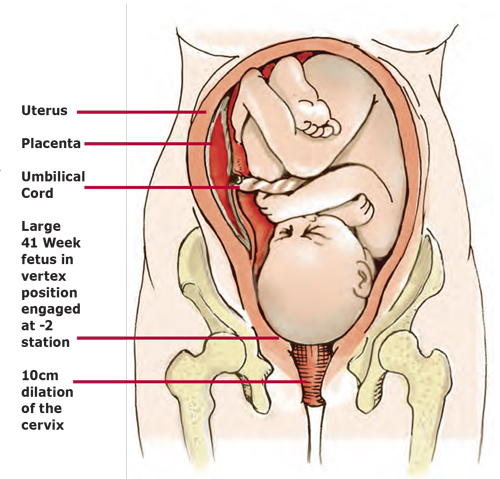
To help guarantee a successful and unremarkable delivery, the baby needs the maximum amount of space in the mother’s uterus and pelvis at exactly the time it is needed. The baby will make a very determined effort to achieve the correct position for birth, but can face resistance if a mother is unaware or unsure of her role in assisting the baby throughout the process. The third trimester of pregnancy, commencing at seven months gestational age, heralds the perinatal period. This critical stage is of greatest concern due to the propensity for adversity in the fetal presentation, position, and attitude.
The biomechanical implications affecting fetal well-being during the third trimester, and for the preparatory phase for labor and delivery, embrace any fetal alignment other than the optimal longitudinal lie, vertex presentation, and flexion attitude. Fetal positioning during the third trimester is not only crucial to an uneventful delivery but possibly to the final construction of the baby’s posture from adolescence through adulthood.