SI joint syndrome continued its fall from fashion due to the lack of reliable clinical studies confirming its very existence. Although many manual therapists quietly continued treating this disorder with some success, no one was able to put forward a convincing biomechanical theory explaining how the sacrum becomes stuck “crooked” between the two innominate bones. Physicians were reluctant to envision a joint with so little movement causing so much pain, while manual therapists countered that its limited motion was vital to proper lumbar spine functioning.
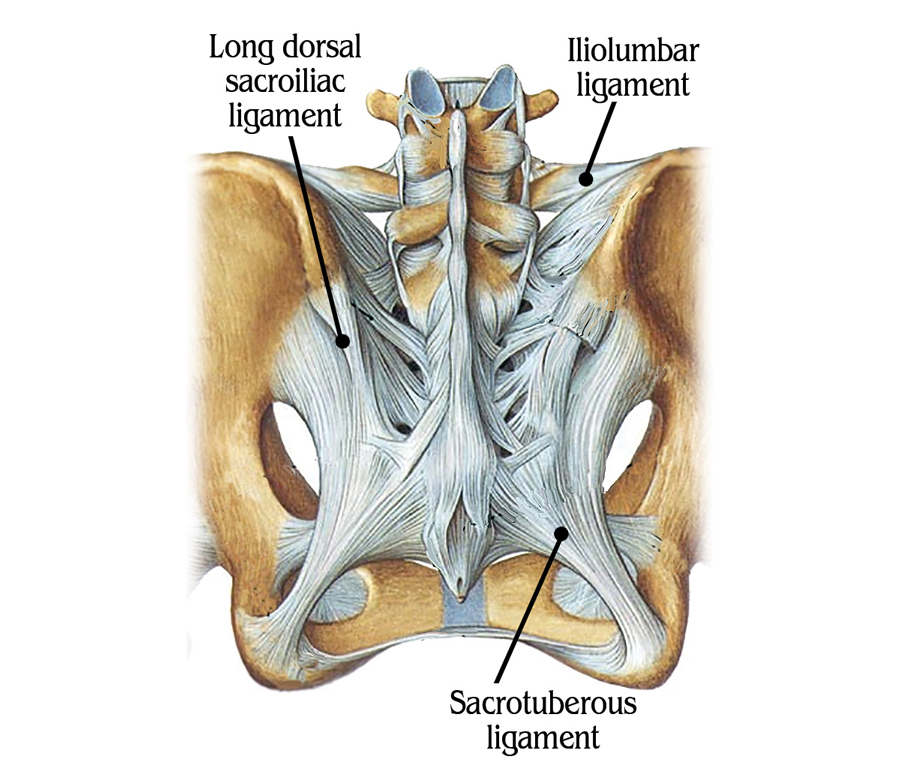
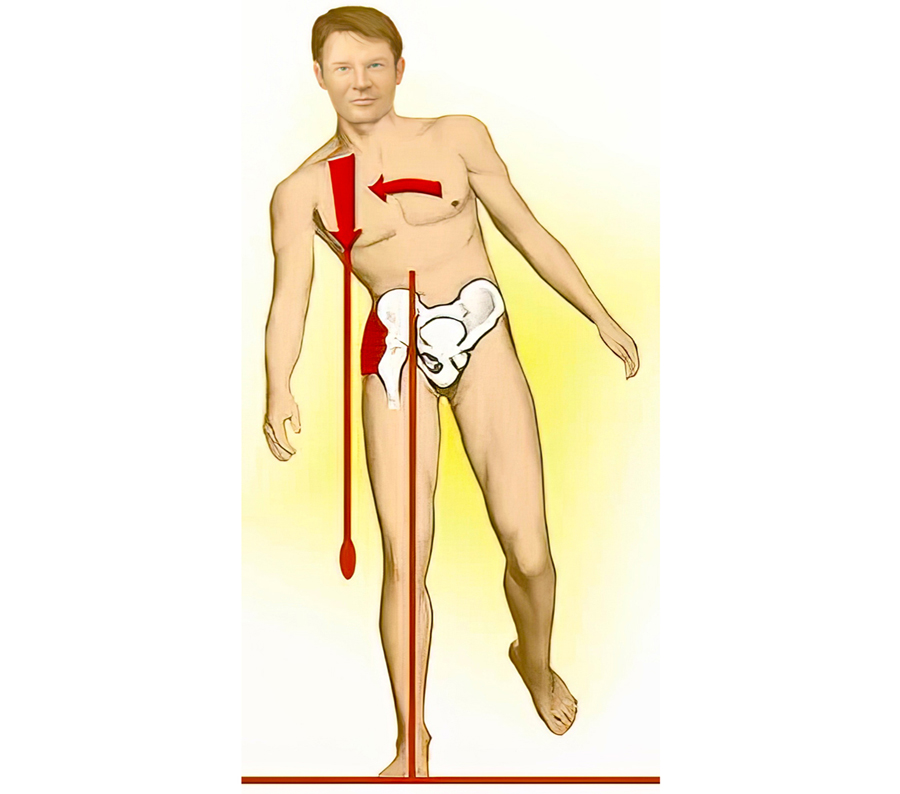
Since most SI joints only move about 2 to 4 millimeters during weight bearing and forward bending, they are described as a gliding-type joint. This motion is quite different from the hinge-type articulation at the knee or the ball-and-socket motion of the hip. Considered a viscoelastic joint, the SI’s major movement comes from ligamentous stretching (Image 1.). Therefore, its primary function within the pelvic girdle is to provide shock absorption for the spine by stretching in various directions. When sacroiliac joints work in perfect harmony with the third bony articulation of the pelvis (symphysis pubis), a marvelous self-locking mechanism develops that helps us walk. Aided by power generated by the hip abductors (gluteus medius/ minimus, TFL and piriformis), the pelvic joints brace the weight-bearing side during gait. This locking system, termed force closure, allows smooth transference of body mass from one leg to the other (Image 2.).
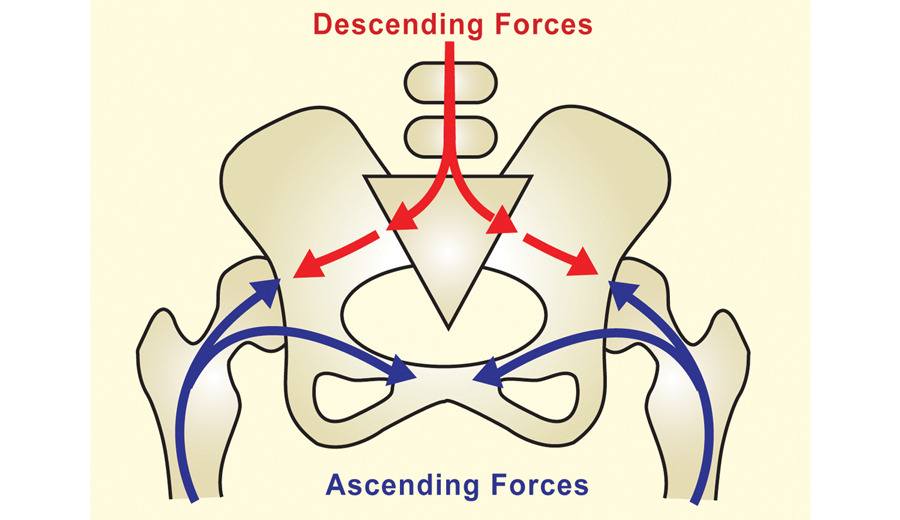
Although no muscles directly bind down the three pelvic joints, when working synchronously with the SI ligaments they provide the pelvis − “the great adapter” – with a remarkable antigravity spring system that can absorb both ascending and descending forces (Image 3.).
Sacroiliac pain tends to be low down; often more to one side, and may extend into the buttock, back of the thigh, and occasionally the calf. It can start suddenly, but in chronic cases, strained joint and ligament mechanoreceptors trigger protective muscle spasm that cause dull, nagging buttock pain or pins and needles down the posterior thigh.
During the aging process, there is decreased motion at the sacroiliac joint due to normal wear and tear and accompanying calcification. This is a perfect example of how the body’s innate wisdom will sacrifice “complexity of motion for stability.” An interesting note is that the age with highest incidence of disabling back pain (25-45 years) is the same age at which the greatest amount of motion is available in the sacroiliac joints. It’s not uncommon for SI joints to stiffen and permanently lock with age. So, it behooves massage therapists to begin incorporating specialized soft-tissue SI joint mobilization maneuvers to help calm the nervous system, relieve protective guarding, and encourage stability and more functional movement through the pelvis. Image 4.
Ligamentous laxity can also be a problem. Traumatic blows to the hip may result in SI joint ligament hypermobility, and over-stimulation of the joint’s mechanoreceptors. As the articulating joint surfaces become jarred loose, ligament microtearing may create an inflammatory response. As sensitized chemoreceptors and mechanoreceptors bombard the spinal cord and brain with noxious stimuli, the brain may choose to layer the area with protective muscle guarding to prevent further insult. This is the beginning of a therapeutically challenging pain/spasm/pain cycle that often is hard to break. It is possible, however, to down-regulate the pain emanating from hypermobile joints by first restoring proper pelvic alignment using techniques such as the one shown in Image 5., and then addressing core strength issues via home retraining exercises.
Femoroacetabular, SI and Lumbar Spinal Joints
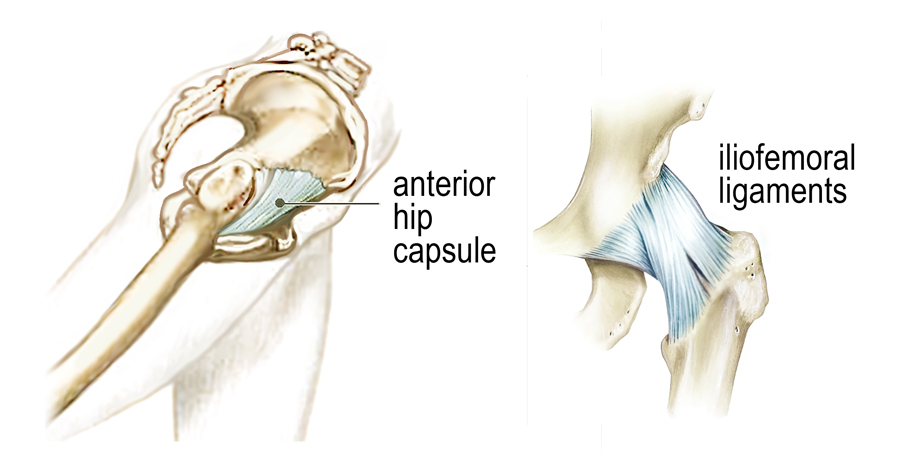
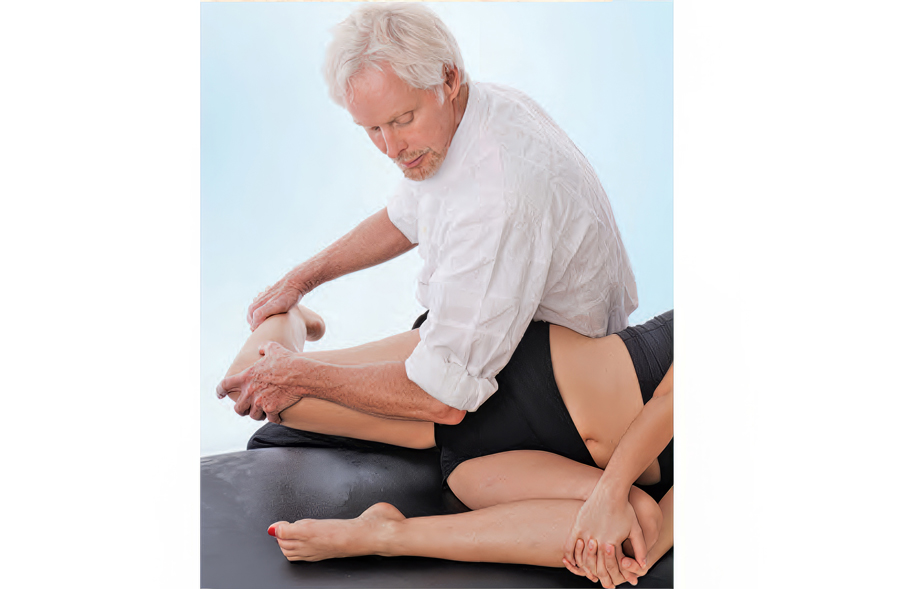
Although the three bones of the pelvis frequently are at the seat of a “primary” lesion, I’ve found that a missing key in successful correction of SI pain is mobilizing motion-restricted femoroacetabular (hip) joints. For the pelvis to effectively absorb the forces imposed upon it, the hips must be aligned and functioning properly. Normally, it’s not the gross motions creating dysfunction within the hip’s truncated joint capsule, but restrictions of minor movements caused by such things as iliofemoral ligament adhesions (Image 6.). Therefore, a rational treatment approach would begin with mobilization of the adhesive anterior hip capsule as shown in Image 7., followed by the iliosacral and sacroiliac alignment techniques presented above.